Pediatrics Review – Emma Holliday Ramahi – Flashcards

Unlock all answers in this set
Unlock answersquestion
What does the APGAR tell you?
answer
General info about how the newborn tolerated labor (1min) and the newborn's response to resuscitation (5min)
question
What does the APGAR not tell you?
answer
What to do next (does not guide therapy) How the baby will turn out (does NOT predict neurologic outcome)
question
PE: When assessing Moro on an LGA newborn, the right arm remains extended and medially rotated.
answer
Erb-Duchenne C5-C6. (Klumpke is C7-C8 + T1) Refer if not better by 3- 6mo for neuroplasty
question
PE: When palpating the clavicles on a LGA newborn, you feel crepitus and discontinuity on the left.
answer
Clavicular Fracture. Will form a callus in 1wk. No tx needed. Can use figure of 8 splint.
question
"Edema. Crosses suture lines."
answer
Caput succedaneum
question
"Fluctuance. Doesn't cross suture lines."
answer
Cephalohematoma
question
answer
Mongolian Spots
question")
answer
Nevus Simplex (Salmon Patch)
question
answer
Milia
question
Appears in up to half of newborns carried to term, usually between day 2-5 after birth. Resolves within first two weeks of life, and frequently individual lesions will appear and disappear within minutes or hours. It is a benign condition thought to cause no discomfort to the baby
answer
Erythema toxicum
question
answer
Strawberry Hemangioma
question
answer
Neonatal Acne
question
"an area of alopecia with orange colored nodular skin" Remove before adolescence b/c it can undergo malignant degeneration.
answer
Nevus Sebaceous
question
"thick, yellow/white oily scale on an inflammatory base". What to do? Gently clean w/ mild shampoo
answer
Seborrheic Dermatitis
question
Two disorders screened for in every state because they are disastrous if not caught early (and happen to be a contraindication to breast feeding...)
answer
Phenylketonuria and Galactosemia.
question
Galactosemia.
answer
Deficient G1p-uridyl- transferase. G1p accum to damage kidney, liver, brain. • Sxs = MR direct hyperbili ; jaundice, ?glc, cataracts, seizures. • Predisposed to E. coli sepsis. • No lactose por vida.
question
Phenylketonuria.
answer
• Deficient Phe hydrolxalase. • Sxs = MR, vomiting, athetosis, seizures, developmental delay over 1st few mos • Signs = fair hair, eyes, skin, musty smell. • Low Phe diet.
question
3 days old, bili @ 10, direct is 0.5. Eating ; pooping well.
answer
Physiologic Jaundice. Gone by 5th DOL. Liver conjugation not yet mature.
question
7 days old, bili @ 12, direct is 0.5. dry mucous membranes, not gaining weight.
answer
Breast feeding Jaundice. ?feeding = dehydration = retain meconium ; re- absorb deconjugated bili.
question
14 days old, bili @ 12, direct is 0.5. Baby regained birth weight, otherwise healthy.
answer
Breast milk Jaundice. Breast milk has glucuronidase and de-conj bili.
question
1 day old, bili @ 14, direct is 0.5. Are you worried? Next best test? If positive? If negative?
answer
Pathologic Jaundice = on 1st DOL, bili ;12, d-bili ;2, rate of rise ;5/day. Test: Coombs Positive: Rh or ABO incompatability Negative: twin/twin or mom/fetus transfusion, IDM, spherocytosis, G6p-DH deficiency, etc.
question
7 days old. Dark urine, pale stool. Bili @ 12, dbili is 8. LFTs also elevated.
answer
Biliary atresia. Bile ducts cannot drain bile. Causes liver failure. Need surgery.
question
Other causes of direct hyperbilirubinemia?
answer
Always r/o sepsis! Galactosemia Hypothyroid Choledochal cyst CF Biliary atresia (;2mo)
question
Random inherited causes of indirect hyperbili? (2)
answer
Gilbert - ?glucoronyl transferase level Crigler-Najjar (type1) - total deficiency
question
Random inherited causes of direct hyperbili (2)
answer
Dubin-Johnson Sx - asx, black liver Rotor Sx - NO black liver
question
Why do we care about hyperbilirubinemia?
answer
Indirect bili can cross BBB, deposit in basal ganglia and brainstem nuclei and cause *kernicterus*. (esp if bili is ;20)
question
Treatment for hyperbilirubinemia
answer
Phototherapy (Tbil;20)--> ionizes the uncoj bili so it can be excreted. Double volume exchange transfusion (Tbil>25) if that doesn't work.
question
Baby is born w/ respiratory distress, scaphoid abdomen ; this CXR. • Biggest concern? • Best treatment?
answer
Diaphragmatic hernia Concern: Pulmonary hypoplasia Txt: If dx prenatally, plan delivery at @ place w/ ECMO. Let lungs mature 3-4 days then do surg
question
Baby is born w/ respiratory distress w/ excess drooling. Best Dx test? What else do you look for?
answer
TE- Fistula Dx: Place feeding tube, take xray, see it coiled in thorax Also look for: VACTER associated anomalies- vertebral, anal atresia, cardiac, radial and renal.
question
1 week old baby becomes cyanotic when feeding but pinks up when crying. • What else do you look for?
answer
Choanal Atresia Also look for: CHARGE associated anomalies- coloboma, heart defects, retarded growth, GU anomalies , Ear anomalies and deafness
question
32 wk premie has dyspnea, RR of 80 w/ nasal flaring. - Prenatal Dx? - Pathophys? - Txt?
;img src=;https://chmanchacentro.com/wp-content/uploads/2018/04/rdsprenatal-dx-l-s.jpg; title=;RDS Prenatal Dx: L/S;2, give antenatal betamethasone Pathophys: Surfactant def, can't keep alveoli open. Txt: O2 therapy with nasal CPAP to keep alveoli open; alt=;RDS Prenatal Dx: L/S
answer
RDS Prenatal Dx: L/S;2, give antenatal betamethasone Pathophys: Surfactant def, can't keep alveoli open. Txt: O2 therapy with nasal CPAP to keep alveoli open
question
38 wk LGA infant born by C/S to an A2GDM has dyspnea/grunting - Pathophys? - Prognosis?
answer
TTN Pathophys: Lung fluid not squeezed out, retained Prognosis: Usually minimal O2 needed. Self resolves in hrs to days
question
41 wk AGA infant was born after ROM yielded greenish- brown fluid. *Next best step? *Complications?
answer
Meconium Aspiration Syndrome Next: intubate and suction before stimulation Complications: Pulmonary artery HTN, pneumonitis
question
Defect lateral (usually R) of midline, no sac - Assoc w/ other d/o? - Complications?
answer
Gastroschisis will see high maternal AFP Not usually associated w/ other d/o Complications: May be atretic or necrotic req removal. Short gut syndrome
question
Defect in the midline. Covered by sac. - Assoc w/ other disorders?
answer
Omphalocele Assoc w/ Edwards ; Patau Trisomies, Beckwith Wiedemann Syndrome = big baby w/ big tongue, ?glc, ear pits
question Repair not needed unless persists past age 2 or 3yo")
Defect in the midline. No bowel present. - Assoc w/ other d/o? - Txt?
answer
Umbilical hernia Assoc w/ congenital hypothyroidism. (also big tongue) Repair not needed unless persists past age 2 or 3yo
question
4wk old infant w/ non- bileous vomiting and palpable "olive" - Metabolic complications? - Txt?
answer
Pyloric stenosis Complications: hypochloremic metabolic alkalosis Txt: immediate surgery referral for myotomy
question Assoc w/ Down Syndrome (esp duodenal)")
2wk old infant w/ bileous vomiting. The pregnancy was complicated by poly- hydramnios. - Assoc w/?
answer
Intestinal Atresia (Or Annular Pancreas) Assoc w/ Down Syndrome (esp duodenal)
question
1 wk old baby w/ bileous vomiting, draws up his legs, has abd distension. - Pathophys?
answer
Malrotation and volvulus *Ladd's bands can kink the duodenum Gut fails to rotate 270* counterclockwise around SMA
question
A 3 day old newborn has still not passed meconium. - DDX? (name 2)
answer
Meconium ileus- consider CF if +FH *gastrograffin enema is dx & tx Hirschsprung's- DRE --> exposion of poo. bx showing no ganglia is gold standard
question - Treatment? NPO, TPN (if nec), antibiotics and resection of necrotic bowel - Risk factors? Premature gut, introduction of feeds, formula.")
A 5 day old former 33 weeker develops bloody diarrhea - What do you see on xray? - Treatment? - Risk factors?
answer
Necrotizing enterocolitis - What do you see on X-ray? pneumocystis intestinal (air in bowel wall) - Treatment? NPO, TPN (if nec), antibiotics and resection of necrotic bowel - Risk factors? Premature gut, introduction of feeds, formula.
question
A 2mo old baby has colicky abd pain and current jelly stool w/ a sausage shapend mass in the RUQ.
answer
Intussusception *Barium enema is dx and tx
question
Newborn male with no palpable testes. - Where are they usually? - Next best test? - When to do surgery?
answer
Cryptorchidism Assoc w/ prune belly syndrome - Where are they usually? Inguinal canal - Next best test? US if not palpable - When to do surgery? If not descended by 1yr to avoid sterility/cancer
question
Newborn male with urethral opening on the ventral surface. - What do you NOT do?
answer
Hypospadias DON'T circumcise! Foreskin is used in eventual repair
question
Newborn child with ambiguous genitalia. One month later has vomiting & ?Na ?K and acidosis. - Most common Cause? - Definitive test? - Tx?
answer
Congenital Adrenal Hyperplasia - Most common Cause? 21 Hydroxylase deficiency. (autosomal recessive) - Definitive test? 17-OH progesterone before and after ACTH bolus - Tx? Hydrocortisone and fludrocortisone (? doses in times of stress)
question
Mothers with pre-existing diabetes (esp type 1) - Prenatal care? - Risks to fetus?
answer
- Prenatal care? Control glc in the 1st trimester & take 4mg folate/day - Risks to fetus? Placental insufficiency/IUGR, Congenital heart dz, NTD, Caudal regression syndrome, Small left colon syndrome
question
Risks of infants born to mothers with gestational diabetes
answer
- LGA. ?risk of birth trauma (clavicle, Erbs), C/S & TTN - Hypoglycemia. Why? Maternal hyperglycemia --> fetal hyperinsulinemia. Complications? Neonatal seizure (always check glc!). Treatment? Feed frequently if <40. IV dextrose if ?EPO. Complications? Renal or splenic vein thromboses - Jaundice. More RBCs to bread down. Risk for kernicterus - RDS. ?insulin interferes w/ cortisol surge prior to birth that normally stimulates lung maturation. Check L/S ratio >2
question
baby 100.4
answer
Sepsis until proven otherwise
question
Sepsis workup in neonate
answer
CBC w/ diff, CXR, blood cultures, urine cultures (use catheter), LP
question
Risk factors for neonatal sepsis?
answer
Prematurity, chorioamnionitis, intrapartum fever, maternal leukocytosis, prolonged rupture of membranes (>18hrs), GBS+ mom.
question
Most common neonatal sepsis bugs?
answer
Group B Strep E. Coli Lysteria monocytogenes
question
Empiric txt for neonatal sepsis?
answer
Ampicillin + Gentamicin until 48hr cx are negative Cefotaxime + Ampicillin if meningitis suspected
question
Maculopapular rash on palms and soles, snuffles, periostitis. Txt?
answer
Syphilis Tx w/ PCN
question
Hydrocephalus, intracranial calcifications and chorioretinitis. Txt?
answer
Toxoplasmosis Tx w/ sulfadiazine + leucovorin.
question
Cataracts, deafness and heart defects (esp PDA, VSD), extramedullary hematopoeisis. Txt?
answer
Rubella No tx.
question
Microcephaly, periventricular calcifications, deafness, thrombo- cytopenia and petechiae. Txt?
answer
CMV Tx w/ ganciclovir, but won't prevent MR
question
Limb hypoplasia, cutaneous scars, cataracts, chorioretinits, cortical atrophy. Txt?
answer
Congenital Varicella if mom infected 1st or 2nd trimester. If mom is exposed 5 days before - 2 days after delivery, baby gets VZIG.
question
Neonatal conjunctivitis: DOL 1-3, red conjunctiva and tearing.
answer
Chemical conjunctivitis caused by silver nitrate drops. Not common anymore b/c we use erythromycin.
question
Neonatal conjunctivitis: DOL 3-5, bilateral purulent conjunctivitis can cause corneal ulceration.
answer
Gonococcal conjunctivitis tx w/ topical erythromycin and IV 3rd gen ceph.
question
Neonatal conjunctivitis: DOL 7-14, red conjunctiva w/ mucoid discharge ; lid swelling
answer
Chlamydia conjunctivitis tx w/ oral erythromycin. Complication is chlamydial pneumonia --> cough, nasal drainage, scattered crackles + bilat infiltrates on CXR
question
A newborn baby has decreased tone, oblique palpebral fissures, a simian crease, big tongue, white spots on his iris - What can you tell his mother about his expected IQ?
answer
Down's Syndrome He will likely have moderate MR. Speech, gross and fine motor skill delay
question
Common medical complications of Down's Syndrome?
answer
- Heart? VSD, endocardial cushion defects - GI? Hirschsprung's, intestinal atresia, imperforate anus, annular pancreas - Endocrine? Hypothyroidism - Msk? Atlanto-axial instability - Neuro? Increased risk of Alzheimer's by 30-35. (APP is on Chr21) - Cancer? 10x increased risk of ALL
question
Omphalocele, rocker-bottom feet/ hammer toe, microcephaly and clenched hand, multiple others.
answer
Edward's syndrome (Trisomy 18)
question
Holoprosencephaly, severe mental retardation and microcephaly, cleft lip/palate, multiple others.
answer
Patau's syndrome (Trisomy 13)
question
14 year old girl with no breast development, short stature and high FSH. Txt?
answer
Turner's syndrome. XO. Most common genotype of aborted fetuses Txt? Estrogen replacement for secondary sex char, and avoid osteoporosis
question
Anomalies assoc w/ Turner's syndrome?
answer
Horseshoe kidney, coarctation of aorta, bicuspid aortic valve
question
18 year old tall, lanky boy with mild MR has gynecomastia and hypogonadism.
answer
Klinefelter's syndrome *increased risk for gonadal malignancy
question
Café-au-lait spots, seizures, large head. Autosomal dominant
answer
Neurofibromatosis
question
Mandibular hypoplasia, glossoptosis, cleft soft palate. W/ FAS or Edwards.
answer
Pierre Robin Sequence
question
Broad, square face, short stature, self- injurious behavior.
answer
Smith Magenis Syndrome Deletion on Chr17
question
Hypotonia, hypogonadism, hyperphagia, skin picking, agression.
answer
Prader-Willi Syndrome Deletion on paternal Chr15
question
Seizures, strabismus, sociable w/ episodic laughter.
answer
Angelman Syndrome Deletion on maternal Chr15.
question
Elfin-appearance, friendly, increased empathy and verbal reasoning ability.
answer
Williams Syndrome Deletion on Chr7.
question
IUGR, hypertonia, distinctive facies, limb malformation, self-injurious behavior, hyperactive.
answer
Cornelia de Lange
question
Microcephaly, smooth philtrum, thin upper lip, ADHD-like behavior. Most common cause of mental retardation.
answer
Fetal Alcohol Syndrome
question
Most common type of MR in boys, Macrocephaly, macro- orchidism, large ears.
answer
Fragile X Syndrome CGG repeats on the X-chr w/ anticipation.
question
Autosomal dominant, or assoc w/ advanced paternal age. Short palpebral fissures, white forelock and deafness.
answer
Waardenburg Syndrome
question
2 y/o M w/ multiple ear infxns, diarrheal episodes & pneumonias. No tonsils seen on exam. - Labs?
answer
Bruton agammaglobulinemia - x-linked - infx start @ 6-9mo - Absence of B cells on flow cytometry - low levels of all Igs
question
17 y/o F with decreased levels of IgG, IgM, IgE, and IgA but normal numbers of B cells.
answer
Combined variable immune deficiency. (acquired)
question
Complication of Combined variable immune deficiency?
answer
Increased lymphoid tissue--> increased risk for lymphoma
question
Most common B-cell defect. Recurrent URIs, diarrhea.
answer
Selective IgA deficiency
question
Complication of Selective IgA deficiency?
answer
Anaphylaxis reaction if given blood containing IgA
question
3wk old M with seizure, truncus arteriosus, micrognathia.
answer
DiGeorge Syndrome
question
Genetic defect of DiGeorge Syndrome?
answer
Microdeletion on Chr22
question
Types of childhood infections in DiGeorge Sx?
answer
Candida viruses PCP pneumonia
question
Infant w/ severe infxns, no thymus or tonsils. Severe lymphopenia.
answer
SCID. See infxns w/ bacterial, viral and opportunistic bugs.
question
SCID inheritance? Txt?
answer
Most common inheritence is XLR. AR is ADA deficiency. Pediatric emergency! Need bone marrow transplant by age 1 or death.
question
3 y/o M child w/ recurrent swollen, infected lymph nodes in groin and staph aureus skin abscesses.
answer
Chronic granulomatous disease XLR. PMNs can ingest but not kill catalase + bugs.
question
How to dx CGD?
answer
Nitrotetrazolium blue (yellow means they have the dz). New test is Flow cytometry w/ DHR-123
question
18mo M baby w/ severe ezcema, petechiae, and recurrent ear infxns.
answer
Wisckott-Aldrich Syndrome. Often present w/ prolonged bleeding after circumcision. Low IgM, high IgA and IgE, slightly low IgG.
question
Newborns lose 10% of birth weight in 1st week. Why? Should regain BW by? Should double weight by? Should triple weight by?
answer
Diuresis of extravascular fluid • Should regain birth weight by? 2wk • Should double weight by? 6mo • Should triple weight by? 1yr
question
Newborns increase 50% of length by? Double length by?
answer
increases 50% by 1 year doubles by 5 years
question
Contraindications to breastfeeding.
answer
Galactosemia, PKU, HIV, HSV on the breast, chemo, Li, Iodide, alcohol.
question
Nutritional characteristics of Breast milk vs. Formula
answer
Breast milk is - whey dominant - more lactose - more LCFA - less Fe but its better absorbed
question
14 y/o boy, always been below 5% in height. Parents are tall & were "late bloomers". Bone age < Real age.
answer
Constitutional Growth Delay Child is likely to have normal final adult height.
question
14 y/o boy, always been below 5% in height. Father is 5'2" and mom is 4'10" Bone age = Real age.
answer
Familial Short Stature
question
14 y/o boy, 50% in height, 97% for weight.
answer
Obesity Bone age ; Real age.
question
Bone age ; Real age.
answer
Obesity Precocious puberty CAH Hyperthyroidism
question
14 y/o boy, starts out in 50% for height, in the past 2 years is now between the 5%-10%. Other risks to consider?
answer
Pathologic Short Stature Craniopharyngioma (vision problems, chect CT) Hypothyroidism (check TFTs) Hypopituitarism (check IgF1) Turners (check karyotype).
question
Primitive Reflex: When head is extended, arms and legs both flex.
answer
Moro Reflex From birth - 4/6mo
question
Primitive Reflex: When you place your finger in palm, flexes hand.
answer
Grasp From birth - 4/6mo
question
Primitive Reflex: Rub cheek, head turns to that side
answer
Rooting. From birth - 4/6mo
question
Primitive Reflex: When stimulate dorsum of foot, steps up.
answer
Placing. From birth - 4/6mo
question
Primitive Reflex: When neck is turned to one side, opposite arm flexes and ipsilateral arm extends
answer
Tonic neck. From birth - 4/6mo
question
Primitive Reflex: When a fall is simulated, arms are extended.
answer
Parachute. From 6-8mo - por vida
question
CNS origin of primitive reflexes?
answer
Brainstem and vestibular nuclei
question
Milestones: Roll over?
answer
6mo. Also, sits w/ support, creep/crawl, stranger anxiety.
question
Milestones: Skips ; copies a triangle?
answer
60mo. Also draws a person w/ 8-10 parts.
question
Milestones: Walk alone?
answer
15mo. Also, builds 3 cube tower and scribbles w/ crayon.
question
Milestone: Walk upstairs w/ alternating feet?
answer
30mo. Also, stands on 1 foot, knows name, refers to self as "I"
question
Milestones: Copy cross and square?
answer
48mo. Also, hops on 1 foot, throws ball overhead, group play and goes to toilet alone.
question
Milestones: Sit unsupported + Pincer grasp?
answer
9mo. Also, walks w/ hand held, object permanence, peak-a-boo ; bye-bye
question
Milestones: walks downstairs, copies a circle, con jump w/ both feet?
answer
36mo. Also, knows age and sex. Understands taking turns. Counts to 3.
question
Milestones: 1?2 of speech is comprehensible ; 2-3word sentences?
answer
24mo. Also, runs well, builds 7 cube tower, holds spoon, helps undress.
question
Milestones: Social smile, start to coo?
answer
2mo. Also, sustains head in plane of body, follows an object 180deg, some vowel sounds
question
Urinary continence should be attained by?
answer
5yo
question
Enuresis: medical causes to r/o?
answer
UTI (do a UA) Constipation (disimpact) Diabetes (check sugar)
question
Txt of enuresis
answer
Primary if continence never achieved, Secondary if after a 6mo period of dryness. *1st* - behavioral- reward system, pee before bed, bell- alarm pad. *2nd* - pharmacological- DDAVP or imipramine
question
Fecal continence should be attained by?
answer
4yo
question
Most common cause of fecal incontinence?
answer
constipation, fecal retention Txt: Disimpact, stool softeners, high fiber diet Behavioral modification: post-prandial toilet sitting
question
Immunizations: birth
answer
HepB (remember to give HepBIV if mom is HbsAg +)
question
Immunizations: 2mo, 4mo, 6mo
answer
HepB (3) Rotavirus (2-3) Dtap (3) HiB (2-4) PCV (4) IPV (4) +flu (starting at 6mo)
question
Contraindications to flu shot?
answer
Egg allergy, also CI for yellow fever vac
question
Immunizations: 12mo
answer
MMR Varicella HepA (live vaccines not for kiddos;12mo) Also maybe: 3rd HBV 3rd Hib 4th PVC13 3rd IPV + flu
question
Contraindications to MMR
answer
Neomycin or streptomycin allergy
question
Immunizations: before 2yo
answer
4 of 5 DTaP 3 of 4 IPV 1 of 2 MMR 1 of 3 Varicella +flu Completed: 3 HepB 2-3 Rotavirus 3-4 Hib 4 PVC13 2 HepA (6mo after the 1st one)
question
Immunizations: before kindergarten
answer
Last of: IPV (4) Dtap (5) MMR (2) Varicella (2) +flu
question
Immunizations: 12yo
answer
1st Tdap booster 1st meningococcal vaccine 1st HPV
question
SYSTOLIC, ;II/VI, soft, vibratory and musical, heard best @ lower mid-sternum
answer
Stills murmur - benign
question
best heard in anterior neck, disappears when jugular vein is compressed.
answer
Venous hum - benign
question
Characteristics of abnormal heart murmurs
answer
- Anything DIASTOLIC. - Anything ;II/VI -; Get an echo
question
Newborn is cyanotic @ birth, O2 does not improve
answer
Transposition of great arteries
question
Transposition of great arteries: - Common in? - Murmur? - Txt?
answer
- Most common in infants of DM mom - Associated murmur: NONE! (unless PDA or VSD) - Immediate tx: PGE1 to keep PDA patent
question
2yo who gets cyanotic and hypernea while playing, squats down
answer
Tetralogy of Fallot
question
Tetralogy of Fallot: - tetralogy? - Murmur? - Txt?
answer
+ Pulmonary stenosis + RA hypertrophy + Over riding aorta + VSD - Murmur: Harsh SEM + single S2 - Txt: O2 and knee-chest position, surgical correction
question
Bipolar woman gives birth to a child w/ holosystolic murmur worse on inspiration.
answer
Ebstein Anomaly Tricuspid insuficciency 2/2 TV displacement into RV.
question
Arrhythmia associated w/ Ebstein Anomaly?
answer
Wolff-Parkinson-White
question
Cyanosis @ birth with holosystolic murmur, depends on VSD or ASD for life. EKG shows LVH. Txt?
answer
Tricuspid atresia. Give PGE1 until surgery
question
Heart defect associated with DiGeorge syndrome. CXR shows ?pulm blood flow and bi-ventricular hypertrophy. Txt?
answer
Truncus arteriosis. Eisenmenger develops early. Do surg in 1st few weeks of life
question
#1 congenital heart lesion. Harsh holosystolic murmur over LL sternal border, loud P2.
answer
Ventriculoseptal defect Most close by 1-2yr
question
VSD: When is surgery indicated? Is louder better or worse?
answer
FTT, 6-12mo w/ pHTN, ;2yrs w/ Qp/Qs ;2:1 Louder is Better. It means the defect is small. Most often membranous. More likely to spontaneously close.
question
Loud S1 w/ fixed and split S2. Older child w/ exercise intolerance.
answer
ASD
question
Most common defect in Down Syndrome baby. Fixed ; split S2 + SEM w/ diastolic rumble. Txt?
answer
Endocardial Cushion Defect @ risk for early Eisenmengers. Surgery before pHTN @ 6-12mo.
question
Continuous machine-like murmur w/ bounding pulses and wide pulse pressure.
answer
PDA
question
PDA: Associations?
answer
Prematurity, congenital rubella syndrome
question
PDA: Txt?
answer
If not closed by 1wk, give indomethacin or surgically close
question
Most common defect in Turner's baby. Decreased femoral pulses, "reverse 3 sign", "notching" @ inf rib border 2/2 incr collateral. May see asymmetry in arm BPs
answer
Coarctation of the Aorta
question
15 year old athlete complains of occasional palpations angina and dizziness. Last week he fainted during the 1st inning of his baseball game. - Murmur? - Txt?
answer
HOCM - Murmur: SEM, better w/ ? preload (squat, handgrip) louder w/ valsalva, standing, exercise (?preload) - Treatment of this child: Beta blockers or CCB (no diuretics or dig- why?). Alcohol ablation or surgical myotomy - No sports or heavy exercise!
question
7 year old girl presents with vague chest pain, pain in several different joints over the past few days, and a rash. Her ESR is elevated, and her EKG shows prolongation of the PR interval. - Txt? - Complications?
answer
Acute Rheumatic Fever - Treatment: Oral PCN (erythromycin) for 10 days, then prophylactic till 20 - Complications: Mitral stenosis, (then aortic or tricuspid involvment)
question
In early childhood, suspect it when: failure to thrive (<5th % weight & height), foul-smelling, bulky, floating stools, recurrent respiratory infections and nasal polyps.
answer
Cystic Fibrosis AR, mutation on Chr7, CFTR protein.
question
CF signs at birth?
answer
Meconium ileus = dilated loops, "ground glass", dx/tx with gastrograffin enema Can also see rectal prolapse from chronic diarrhea.
question
CF: Dx? Txt?
answer
Diagnosis? Sweat test--> >60mEq/L chloride is diagnostic Treatment? - For thick resp. secretions? DNAse (mucolytic), albuterol/saline nebs - For pneumonia? Most often pseudomonas or colonized w/ b. cepacia Tx w/ piperacillin + tobramycin or ceftazidime - For pancreatic insuff? Enzy replacement w/ meals + ADEK supplement - For electrolyte loss through skin? Adequate fluid replacement when exercising or when hot.
question
Asthma txt: If pt has sxs twice a week and PFTs are normal?
answer
Albuterol only
question
Asthma Txt: If pt has sxs 4x a week, night cough 2x a month and PFTs are normal?
answer
Albuterol + ICS
question
Asthma Txt: If pt has sxs daily, night cough 2x a week and FEV1 is 60-80%?
answer
Albuterol + inhaled CS + long-acting beta-ag (salmeterol)
question
Asthma Txt: If pt has sxs daily, night cough 4x a week and FEV1 is <60%?
answer
Albuterol + inhaled CS + salmeterol + montelukast and oral steroids
question
Mgmt of asthma exacerbation?
answer
txt w/ inhaled albuterol and PO/IV steroids. Watch peak flow rates and blood gas. PCO2 should be low. Normalizing PCO2 means impending respiratory failure --> INTUBATE.
question
Asthma complications
answer
Allergic Brochopulmonary Aspergillus
question
A 12 y/o girl presents with a 2 day history of vomiting. For the last 4 weeks, she noticed weight loss, polyphagia, polydipsia and polyuria. Na = 130, Cl = 90, HCO3 = 15, glucose = 436. Dx? Pathophys? Next step? Long term txt?
answer
Diabetes • Next best step? Start insulin drip + IVF. Monitor BGL and anion gap. Start K. Bridge w/ glargine once tolerating PO. • Pathophys? T-cell mediated destruction of islet cells, insulin autoAb, glutamic acid decarboxylase autoAb • Long term treatment? Will need insulin tx.
question
Diagnostic criteria for DM?
answer
Fasting glc >125 (twice) 2hr OGTT (75g) > 200 Any glc > 200 + symptoms
question
Dysmorphic RBCs or RBC casts in UA?
answer
glomerular source
question
Definition of nephritic syndrome?
answer
Proteinuria (but <2g/24hrs) hematuria edema azotemia
question
Hematuria 1-2 days after runny nose, sore throat & cough?
answer
Berger's Dz (IgA nephropathy). Most common cause.
question
Hematuria 1-2 weeks after sore throat or skin infxn?
answer
Post-strep GN- smoky/cola urine, best 1st test is ASO titer. Subepithelial IgG humps
question
Hematuria + Hemoptysis?
answer
Goodpasture's Syndrome. Abs to collagen IV
question
Hematuria + Deafness?
answer
Alport Syndrome. XLR mutation in collagen IV
question
Best test for kidney stones?
answer
CT
question
Nephrolithaisis: Most common type?
answer
Calcium oxalate Txt w/ HCTZ
question
Nephrolithiasis: Kid w/ family hx of stones. Type?
answer
Cysteine. Can't resorb certain AA.
question
Nephrolithiasis: Chronic indwelling foley and alkaline pee?
answer
Mg/Al/PO4 = struvite Proteus, Staph, Pseudomonas, Klebsiella
question
Nephrolithiasis: If leukemia being treated w/ chemo?
answer
Uric Acid Txt by alkalinizing urine + hydration
question
Nephrolithiasis: s/p bowel resection for volvulus
answer
Pure oxalate stone. Ca not reabsorbed by gut (pooped out)
question
Nephrolithiasis Treatment? - Stones 2cm? - Stones 5mm-2cm?
answer
- Stones Will pass spontaneously. Just hydrate - Stones ;2cm --> Open or endoscopic surgical removal - Stones 5mm-2cm --> Extracorporal shock wave lithotropsy
question
Best initial test for proteinuria
answer
Repeat test in 2 weeks, then quantify w/ 24hr urine
question
Definition of nephrotic syndrome?
answer
;3.5g protein/24hrs hypoalbuminemia edema hyperlipidemia (fatty/waxy casts)
question
Most common cause of nephrotic sx in kids? Txt? Complications?
answer
Minimal change dz - fusion of foot processes - Treat with prednisone for 4-6wks. - Most common complication is infection- Make sure immunized against pneumococcus and varicella.
question
nephrotic patient suddenly develops flank pain?
answer
Suspect renal vein thrombosis! 2/2 peeing out ATIII, protein C and S. Do CT or U/S stat!
question
An African American (or Mediterranean) kid w/ sickle cell disease comes in...Swollen, painful hands and feet.
answer
Dactylitis. 2/2 necrosis of small bones
question
An African American (or Mediterranean) kid w/ sickle cell disease comes in...Excruciating pain in the extremities, ulcers, hip pain.
answer
Pain crises. Ischemic damage 2/2 sickling
question
An African American (or Mediterranean) kid w/ sickle cell disease comes in...Point tenderness on femur, fever, and malaise.
answer
Osteomyelitis. Most common bug is Salmonella
question
?retics, nl MCV sickles, targets, HJ bodies
answer
Sickle cell blood smear
question
An African American (or Mediterranean) kid w/ sickle cell disease comes in...Acute drop in HCT with ??retics?
answer
Aplastic crisis. Parvo B19
question
An African American (or Mediterranean) kid w/ sickle cell disease comes in...Recurrent RUQ pain after meals.
answer
Pigment gallstones. Do Chole.
question
An African American (or Mediterranean) kid w/ sickle cell disease comes in...Respiratory distress ; emergent tonsilectomy?
answer
Waldyer Ring hyperplasia.
question
An African American (or Mediterranean) kid w/ sickle cell disease comes in...Proteinuria and increased creatinine + recurrent UTIs?
answer
Kidney infarcts due to sickled RBCs
question
Most common cause of sepsis in sickle cell pts?
answer
Strep Pneumo
question
Sickle cell pt presents w/ fever, cough, chest pain, chills, and SOB? Txt?
answer
Acute Chest syndrome. Pulmonary infarction. Most common cause of death. Txt: O2, Abx, exchange transfusion
question
Sickle cell pt p/w acute confusion and focal neurologic deficits? Txt?
answer
Stroke Txt: Exchange transfusion (NOT tPA!) Assessing risk? Transcranial doppler (v ;200cm/sec), keep HbS ;30%
question
Sickle cell Vax and ppx?
answer
*23-valent pneumococcal vaccine* @2yo H. flu *N. meningitides* +PCN prophylaxis from 2mo-6yo
question
If sickle cell pt p/w fatigue and megaloblastic anemia? Txt?
answer
Most likely folate deficiency (higher need 2/2 ?retics) Txt: Hydroxyurea increases production of HbF. Treat infx aggressively and manage pain. Bone marrow transplant cures, but has 10% post op mortality
question
Normal instances of childhood anemia?
answer
Physiologic drop in H;H 2-3mo Transient Erythroblastopenia 3mo-6yo - immune suppression after viral infection (not B19)
question
18 mo kiddo, picky eater, drinks lots of cow's milk. ?H&H, MCV 75, ?ferritin, ?TIBC
answer
Fe-deficiency. Tx w/ oral ferrous salts.
question
18 mo kiddo, eats a varied diet. Mom is Italian. ?H&H, MCV 60, ?RDW
answer
Thalassemia. Varying degrees. Tx w/ transfusion & deferoxamine. Can see expanded medullary space
question folate. Tx w/ daily folate.")
8 mo kiddo is irritable, has glossitis & FTT. Picky eater, drinks lots of goat's milk.
answer
Folate-deficiency. See low serum (RBC) folate. Tx w/ daily folate.
question
4mo pale baby, normal plts and WBCs but hemaglobin is 4. Increased RBC ADA and low retics. Triphalangeal thumbs. Txt?
answer
Blackfan-Diamond Anemia Txt: Corticosteroids, transfusions, stem cell transplant.
question
18mo baby presents w/ low plts, low WBCs, and profound anemia. He has café-au-lait spots, microcephaly, and absent thumbs. Dx? Txt?
answer
Fanconi Anemia - Dx? Bone marrow shows hypoplasia, Cytogenetic studies for chr breaks - Tx? Corticosteroids, androgens, bone marrow transplant.
question
Complications assoc w/ Fanconi Anemia
answer
Increased risk for AML and other cancers.
question
2 y/o baby presents w/ hyperactivity, impaired growth, abdominal pain and constipation. Dx?
answer
Lead poisoning Dx: venous blood sample, check lead level
question
Txt for lead poisoning
answer
Check venous blood level ;45 Txt w/ Succimer ;70 admit and txt w/ EDTA + Dimercaprol
question
Lead poisoning screening?
answer
Test blood lead levels btw 12-24mo if low SES or lives in an old house (;1960)
question
15 y/o F recurrent epistaxis, heavy menses ; petechiae. ?plts only. Txt?
answer
ITP Tx w/ IVIG for 1-2 days, then prednisone, then splenectomy. NO plts!!
question
15 y/o F recurrent epistaxis, heavy menses, petechiae, normal plts, ? bleeding time and PTT. Txt?
answer
VWD DDAVP for bleeding or pre-op. Replace factor VIII (contains vWF) if bleeding continues.
question
7 y/o M recurrent bruising, hematuria, ; hemarthroses, ? PTT that corrected w/ mixing studies* Txt?
answer
Hemophilia If mild, tx w/ DDAVP, otherwise replace factors.
question
1wk old newborn, born at home, comes in with bleeding from the umbilical stump ; bleeding diathesis. Txt?
answer
VitK def ? II, VII, IX and X (Same as CF kid with malabsorbtion) Txt: FFP acutely + vitK shot
question
9 y/o F with Wilson's disease developed fulminant liver disease. 1st factor depleted? 2 factors not depleted?
answer
1st: VII, so PT increases 1st Not: VIII and vWF b/c they are made by endothelial cells.
question
A 3 y/o child is brought in with petechiae, abdominal pain, vomiting and lethargy. He had bloody diarrhea 5 days ago after eating hamburgers at a family picnic. Labs reveal thrombocytopenia and ?creatinine
answer
Hemolytic Uremic Syndrome
question
Most common cause of HUS?
answer
*E. Coli O157H7* Shigella Salmonella Campylobacter
question
Txt for HUS?
answer
NO platelets! Tx w/ aggressive nutrition (TPN) and early peritoneal dialysis. Don't give abx for bloody diarrhea. Can ? risk of HUS
question
A 5 y/o child is brought in with purpura on his legs and buttocks, abdominal pain, joint pain, current jelly stool. His smear appears normal, as are his coagulation studies and electrolytes. IgA and C3 are deposited in the skin.
answer
Henoch Schonlein Purpura Most common cause? Usually follows URI Treatment? Symptomatic treatment. Can use steroids for GI or renal dx.
question
New onset seizure, ataxia and HA worse in the AM with vomiting for a month.
answer
Brain tumor. Most likely infratentorial
question
Most common childhood brain tumor?
answer
Pilocytic astrocytoma of cerebellum. Resect:~90% survive
question
2nd most common childhood brain tumor?
answer
Medulloblastoma. Vermis, obstruct 4th V
question
Adolescent with height in 5th %, w/ bitemporal hemianopsia. See calcifications in sella turcica.
answer
Craniopharyngioma Suprasellar A remnant of Rathke's pouch.
question
2 year old hypertensive child with asymptomatic abdominal mass. Workup? Associations? Txt?
answer
Wilm's tumor Best test: Abdominal CT. Do CXR to check lung involvement Assoc w/ Aniridia, GU anoms, Hemihypertrophy, Beckwith-Weidemann Txt: Surgery, chemo, rads
question
4 year old with jerking movements of eyes and legs, bluish skin nodules and a tender abdominal mass Diagnostic tests?
answer
Neuroblastoma ?urine homovanillic or vanillylmandelic acid.
question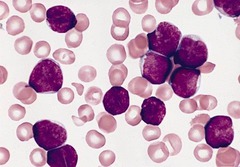 ;30% lymphoblasts Txt: VDP + CNS tx w/ intrathecal methotrexate Poor prognostic factors: 10, ;100K WBC" alt="ALL Best test: Bone marrow biopsy--> >30% lymphoblasts Txt: VDP + CNS tx w/ intrathecal methotrexate Poor prognostic factors: 10, >100K WBC">
;30% lymphoblasts Txt: VDP + CNS tx w/ intrathecal methotrexate Poor prognostic factors: 10, ;100K WBC" alt="ALL Best test: Bone marrow biopsy--> >30% lymphoblasts Txt: VDP + CNS tx w/ intrathecal methotrexate Poor prognostic factors: 10, >100K WBC">
3 year old girl w/ a limp ; left leg pain, T99.9, HSM, petechiae, ; pallor. Cells are CALLA and TdT +. Best test? Txt? Prognosis?
;30% lymphoblasts Txt: VDP + CNS tx w/ intrathecal methotrexate Poor prognostic factors: 10, ;100K WBC" alt="ALL Best test: Bone marrow biopsy--> >30% lymphoblasts Txt: VDP + CNS tx w/ intrathecal methotrexate Poor prognostic factors: 10, >100K WBC">answer
ALL Best test: Bone marrow biopsy--> >30% lymphoblasts Txt: VDP + CNS tx w/ intrathecal methotrexate Poor prognostic factors: 10, >100K WBC
question
14 y/o boy w/ enlarged, painless, rubbery nodes, drenching fevers, and 10% weight loss. Best test? Txt?
answer
Hodgkin Lymphoma Best test: excisional bx, and then staging CT or laparoscopy to determine txt Txt: chemo + rads, 90% cure if stage I or II
question
7 year old girl with non-productive cough and large anterior mediastinal mass on CXR. Best test? Txt?
answer
Non-Hodgkin Lymphoma Best test: Biopsy of mass, bone marrow bx for staging Treatment: Surgical excision if abdominal tumor. Can use anti-CD20 if B-cell tumor. Rads for some.
question")
2y/o w/ a fever to 105 3 days later gets a pink, maculopap rash on trunk arms and legs.
answer
Roseola (HHV6)
question")
2y/o w/ a low grade fever, lacy reticular rash on cheeks and upper body (spares the palms/soles)
answer
5th Disease/Erythema Infectiosum (Parvovirus B19)
question Txt: PCN prevents rheumatic fever. Won't help reduce changes of APSGN")
Fine, mac-pap desquamating rash begins on chest and spreads to neck, trunk, ; extremities + strawberry tongue. Sore throat 1-2wks prior. Txt?
answer
Scarlett Fever (group A strep) Txt: PCN prevents rheumatic fever. Won't help reduce changes of APSGN
question
Cough, runny nose, fever --> macular rash begins behind ears & spreads down. Gray spots on the buccal mucosa. Txt?
answer
Measles (paramyxovirus) Txt: Vitamin A + supportive care
question
Sore throat, joint pain fever -->pinpoint rash on the face and spreads down. Rose spots on the palate.
answer
Rubella (paramyxovirus)
question")
Baby w/ poor feeding. Vesicles in mouth on palms and soles + rash on buttocks
answer
Hand-Foot-and-Mouth Disease (Coxsackie virus A16)
question
16 year old M with swollen parotid glands, fever & HA. Complications?
answer
Mumps (paramyxovirus) Complications: orchidis and sterility
question 8yo" alt="Lyme Dx (Borrelia burgorferi) Complications: arthritis, heart block, meningitis, Bells palsy Txt: Amoxicillin. Doxycycline if >8yo">
8yo" alt="Lyme Dx (Borrelia burgorferi) Complications: arthritis, heart block, meningitis, Bells palsy Txt: Amoxicillin. Doxycycline if >8yo">
6y kid from central PA who went camping has fever. Complications? Txt?
8yo" alt="Lyme Dx (Borrelia burgorferi) Complications: arthritis, heart block, meningitis, Bells palsy Txt: Amoxicillin. Doxycycline if >8yo">answer
Lyme Dx (Borrelia burgorferi) Complications: arthritis, heart block, meningitis, Bells palsy Txt: Amoxicillin. Doxycycline if >8yo
question
6y/o kid from coastal NC, went camping. Had fever, myalgias, abd pain. Complications? Txt?
answer
Rocky Mountain Spotted fever. (Rickettsia rickettsii) Complications: Vasculitis and gangrene Txt: Doxycycline no matter what age
question
8yo kid, multiple excoriations on arms, itchy at night. Txt?
answer
Scabies Txt: 5% Permetrin for whole household
question
Honey-colored crusted plaque on face. Txt?
answer
Impetigo (most common bug is Staph if bullous) Txt: topical Muciprocin if localized
question
Inflamed conjunctiva and multiple blisters. Nikolsky's + Txt?
answer
Staph Scalded Skin Syndrome from exfoliative toxin Txt: IV Oxacillin or Nafcillin
question
Meningitis bugs in kids? Txt?
answer
Strep Pneumo H. Influenza N. meningitidis Txt: Ceftriaxone and Vancomycin
question
Meningitis bugs in immune suppressed? s/p brain surgery?
answer
Listeria, Txt: Ampicillin Staph, Txt: Vancomycin
question
Txt for roommate of the kid in the dorms who has bacterial meningitis and petechial rash?
answer
Rifampin!!
question
2 y/o w/ fever to 102, tugging on his right ear. Patient's tympanic membrane is red and bulging. Dx? Risk factors? Txt? Complications?
answer
Otitis Media Most sensitive dx test? Limited mobility on insufflation or air-fluid level Risks? ?SES, Native Americans, formula fed, tobacco smoke, around kids Treatment? Amoxicillin or azithromycin for 10days. If no improvement in 2-3 days, switch to amox-clav (augmenting) Complications? Effusion - place tubes if bilat effusion >4mo or if bilateral hearing loss.
question
12y/o in summer swim league has pain when adjusting his goggle straps behind his ear. Thick exudates coming from the ear and tender posterior auricular nodes. Txt? Complicaitons?
answer
Otitis Externa Txt? Topical Ciprofloxacin Complications? Malignant external otitis-->can invade to temporal bone-->facial paralysis, vertigo. Need CT and IV abx. May need surgery
question
7y/o w/ exudative pharyngitis w/ tender cervical lymph nodes and fever of 102. Dx? Txt?
answer
GABHS Pharyngitis Dx: rapid strep antigen, send culture if negative and high clinical suspicion Txt: PCN or Erythromycin to prevent Rheumatic fever
question
A child presents w/ "muffled voice", stridor and refuses to turn her head to the left. Txt? Complications?
answer
Retropharyngeal abscess Txt: I&D for C&S. GAS + anaerobes --> 3rd gen cephalosporins + Ampicillin or Clindamycin Complications: Retropharyngeal space communicates with mediastinum --> mediastinitis
question
A child presents w/ "hot potato voice" and upon throat exam her uvula is deviated to the right 2/2 a bulge. Txt?
answer
Peritonsillar abscess Txt: Aspiration or I&D + Abx Tonsillectomy if recurrent, >5 episodes of Strep/yr for 2yrs, or >3 episodes/yr for 3yrs
question
Older kid w/ sore throat, fever, fatigue, generalized adenopathy and splenomegaly (anterior and posterior cervical nodes). Dx? Txt? Complications?
answer
Epstein-Barr virus Dx: blood smear shows atypical lymphocytes. + Heterophiles Ab (Monospot) test Txt: rest and symptomatic Caution: splenic hemorrhage or rupture (most in 2nd week) -> no contact sports until splenomegaly resolves
question
What happens if you give an EBV pt Ampicillin or Amoxicillin?
answer
Maculopapular rash (immune mediated vasculitic)
question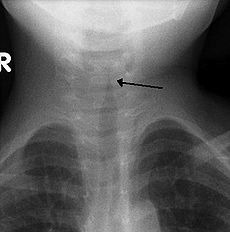
1 y/o w/ fever to 100.5 & "barking" cough and loud noises on inspiration. Bug? Txt?
answer
Croup (Parainfluenza virus) "steeple sign" Txt: mist, epinephrine nebs, steroids
question
2 y/o w/ fever to 104 & drooling w/ intercostal retractions and tripod position. Bug? Txt?
answer
Epiglottitis (H. flu B in unimmunized, Strep pyo, Strep pneumo, Staph) "thumbprint sign" INTUBATE IN OR!!! Txt: anti-Staph Abx + 3rd gen cephalosporin
question
Kid comes in w/ cough productive of yellow-green sputum, runny nose and T100.8. Lung exam only reveals some coarse rhonchi. Txt?
answer
Acute Bronchitis Supportive txt w/ anti-pyretic, tussives, histamines
question
Kid comes in w/ cough productive of yellow-green sputum, runny nose and T100.8. Lung exam reveals decreased breath sounds and crackles in LLL. WBC = 16K. Dx?
answer
Pneumonia Dx: CXR, typical vs atypical
question
Most common cause of pneumonia in neonates <28d?
answer
GBS E coli Listeria
question
Most common cause of pneumonia in 1-3mo?
answer
C. trachomatis RSV Parainfluenzae Strep pneumo
question
Findings specific for chlamydia pneumonia?
answer
Staccato cough eosinophilia
question
Most common cause of pneumonia in kids 4mo-5yo?
answer
VIRAL (RSV) then Strep pneumo
question
Most common cause of pneumonia in kids >5yo?
answer
Mycoplasma Strep pneumo
question
9mo infant w/ runny nose, wheezy cough, T = 101.5, and RR = 60. Retractions are visible and pulse ox is 91%. CXR? Bug? Txt?
answer
Bronchiolitis CXR: hyperinflation w/ patchy atelectasis Bug: RSV, confirm w/ swab Txt: hospitalize if respiratory distress, albuterol nebs, NO steroids Ppx: Palivizumab for premies, CHD, lung dx, immune dx
question
9mo infant with severe coughing spells with loud inspiratory whoops and vomiting afterwards. 2 weeks ago she had runny nose and dry cough. Dx? Bug? Txt?
answer
Whooping cough (Bordetella pertussis) CBC: lymphocytosis Txt: Erythromycin x14d. Treat family members and daycare peers.
question
Anatomic risk factor for UTI?
answer
Vesiculoureteral reflux Give ppx Abx
question
Diagnosis of UTI?
answer
clean catch or cath sample, UA, UCx (>10K CFU) US: any febrile UTI for anatomy, abscess, or hydronephrosis
question
Txt of UTI?
answer
PO Bactrim or Nitrofurantoin
question
Txt of pyelonephritis?
answer
IV Ceftriaxone or Ampicillin + Gentamicin x14d
question
Who needs VCUG s/p UTI?
answer
all males females 5yo w/ 2nd UTI
question
Tc-labeled DMSA scan?
answer
Most sensitive and accurate study of scarring and renal size, but not first line for UTI workup
question
DDx for limp?
answer
Trauma Dev hip dysplasia Legg-Calve-Perthes Dx Transient Synovitis SCFE Osgood-Schlatter JRA Kawasaki
question
18mo F w/ asymmetric gluteal folds on exam. Dx? Txt? Risk factors?
answer
Developmental hip dysplasia Dx: "clunk" on Barlow, US of hip if unsure Txt: Pavilk harness, surgery Risks: 1st born, FHx, breech
question
5 y/o M initially w/ painless limp now has pain in his thigh.
answer
Legg-Calve-Perthes Disease avascular necrosis
question
5 y/o M initially w/ a cold 1wk ago now presents w/ a limp & effusion in the hip. X-rays are normal and ESR is 35 (?), T = 99.8, WBCs = 10K. Txt?
answer
Transient Synovitis Txt: bed rest x1wk + NSAIDS
question
14 y/o lanky M w/ nagging knee pain and decreased ROM of the hip on exam. Txt?
answer
SCFE (Slipped Capital Femoral Epiphysis) Txt: surgically close and pin epiphysis to avoid osteonecrosis
question
14 y/o basketball player has knee pain and swelling of the tibial tubercle.
answer
Osgood-Schlatter overuse injury from jumping
question
12 y/o F w/ 2 wk history of daily fevers to 102 and a salmon colored evanescent rash on her trunk, thighs and shoulders. Her left knee and right knee are swollen. Prognostic factors? Txt?
answer
JRA +ANA good prognostic factor +RF poor prognostic factor (also polyarticular and older age of onset) Txt: NSAIDs > Methotrexate > Steroids
question
2y/o F w/ a 2 wk history of daily fevers to 102 and a desquamating rash on the perineum. She has swollen hands and feet, conjunctivitis and unilateral swollen cervical lymph node. Lab results? Further workup? Txt? Complications?
answer
Kawasaki Dx Labs: ?plts (wk2-3), ? urine WBC, ?LFTs, ?CSF protein Workup: 2D Echo and ECG --> repeat Echo after 2-3wk of txt Txt: IVIG +ASA --> ASA + Warfarin Complications: coronary artery aneurysm or MI
question
Bone pain, F. "Onion skinning" on xray. (layers of periosteal development). Txt?
answer
Ewing sarcoma More common if hx of retinoblastoma or previous radiation. Txt: Rads and/or surgery
question
Bone pain, >10yo, M>F. "Sunburst" and "Codman's sarcoma triangle" on xray. Txt?
answer
Osteogenic sarcoma Txt: Chemo and/or surgery
question
Diffuse bone pain in a pt w/ petechiae, pallor, and increased infections?
answer
Leukemia bone pain can be the presenting sx for leukemia
question
Infant with increasing head size, prominent occiput, cerebellar ataxia and delayed motor development. What will you see in imaging?
answer
Dandy-Walker malformation CT or MRI: Cystic expansion of 4th ventricle. Can see Agenesis of cerebellar vermis.
question
This morning, a 1 y/o develops a fever to 102.4. Four hours later, the parents bring her in after she has a 3-4 minute tonic-clonic seizure. Next best step?
answer
Febrile Seizure Give Acetamenophen. No increased risk for epilepsy
question
An 8 year old boy gets in trouble in school because he is always "staring into space". These episodes last only seconds, have lip smacking, and he goes right about his business after they are done. Imaging? Txt?
answer
Absence Seizure EEG: 3Hz spike and wave discharge Txt: Ethosuxamide or Valproate
question
A 6mo old is brought in for multiple symmetric contraction episodes of neck, trunk and extremities that occur in spells. Imaging? Txt?
answer
Infantile Spasms EEG: Hypsarrhythmia = asynchronous, chaotic, bilateral Txt: ACTH > Prednisone
question
8y/o w/ difficulty w/ balance while walking, no DTRs, bilateral Babinski and "explosive, dysarthric speech". Most common cause of death?
answer
Friedrich Ataxia AR, trinucleotide repeat Most common cause of death is HOCM --> CHF
question
2y/o w/ gait disturbance, loss of intellectual fxn, nystagmus and optic atrophy. Cresyl violet --> metachromatic staining.
answer
Metachromatic leukodystrophy AR, deficiency of Arylsulfatase A --> accumulation of cerebroside sulfate
question
12y/o w/ decreased school performance, behavior changes, ataxia, spasticity, hyperpigmentation, ?K, ?Na, acidosis. Prognosis?
answer
Adrenoleukodystrophy XLR Death w/in 10yrs
question
9mo who had previously been reaching milestones starts to lag. Seizures, hypotonia, cherry red macula.
answer
Tay-Sachs XLR, deficiency of hexosaminidase A --> accumulation of GM2
question
3mo infant lays in the "frog-leg" position, <5th% 2/2 feeding difficulties, hypotonic, fasiculations of the tongue and absent DTRs.
answer
SMA 1-Werdnig-Hoffman Dx most die before age 2yo
question
6y/o is brought in 2/2 "clumsiness" and frequent falls. The lower leg has decreased muscle bulk and appears "stork- like". There are multiple small injuries on the hands and feet. You notice pes cavus and claw hand. Tests? Txt?
answer
Marie-Charcot-Tooth Dx Tests: decreased motor/sensory nerve velocity, dural nerve biopsy. nml CPK Txt: stabilize ankles w/ surgical fusion, usually normal lifespan, most remain ambulatory

