Dermatology Pathology Slides from Lecture – Flashcards

Unlock all answers in this set
Unlock answers
question

What is the type of lesion? A. Macule B. Papule C. Patch D. Plaque E. Ulcer
answer
B. Papule palpable lesion, <10 mm
question
What is the type of lesion? A. Macule B. Papule C. Patch D. Plaque E. Ulcer
answer
C. Patch
question
What is the type of lesion? A. Macule B. Papule C. Patch D. Plaque E. Ulcer
answer
D. Plaque
question

What is the type of lesion? A. Macule B. Papule C. Patch D. Plaque E. Ulcer
answer
E. Ulcer
question

axilla distribution, *burrows*
answer
Scabies
question
*burrows*
answer
Scabies
question
*burrows*; finger web involvement
answer
Scabies
question
RIGHT mite itself MIDDLE poop LEFT cyst
answer
Scabies
question

answer
Nodular Scabies
question
hundred to thousands of mites
answer
Nodular Scabies
question
pustules papulovesicles
answer
Fire Ant Sting
question

nits
answer
Head lice
question
answer
Pubic Louse
question

answer
Body/Head Louse
question

answer
Tick
question
answer
Flea
question
leg involvement not displaying "breakfast, lunch, and dinner" pattern
answer
Flea Bites
question
necrotic ulceration
answer
Brown Recluse Bite (Note that Black Widow bites do not cause cutaneous lesions.)
question
necrotic ulceration
answer
Brown Recluse Bite (Note that Black Widow bites do not cause cutaneous lesions.)
question
purple, polygonal, pruritic papules and plaques commonly seen on the wrists, genitalia, and buccal mucosa
answer
*Lichen Planus* (*Can progress to squamous cell carcinoma.*)
question
purple, polygonal, pruritic papules and plaques *Wickham's striae* (reticulated scaling) on the *buccal mucosa* also seen on the wrists and genitalia
answer
*Lichen Planus* (*Can progress to squamous cell carcinoma.*)
question
"dew drops" without inflammation
answer
Miliaria Crystalina (Caused by occlusion of eccrine sweat ducts and seen in "hot, humid" weather. Note that miliaria *rubra [monomorphic red papules]* and *profunda [with pustules]* are progressively deeper with more inflammation.)
question

keratotic firm flesh-colored to red follicularly based papules seen on lateral arms, thighs, +/- cheeks
answer
Keratosis Pilaris
question
")
flat-topped, asymptomatic, shiny papules seen on arms, dorsal hands, genitalia, and trunk
answer
Lichen Nitidus (Histology demonstrates a characteristic *ball and claw* pattern.)
question

What other body parts does this "like?" A. Eye B. Feet C. Finger D. Mouth E. Scalp
answer
D. Mouth *Lichen planus "likes" the buccal mucosa, specifically.*
question
Name the acne.
answer
Open comedonal (non-inflammatory) (Acne is caused by the gram positive anaerobe **Proprionibacterium acnes**.)
question
Name the acne. ("Are you impressed by it?")
answer
Severe Nodulocystic Acne
question

central facial erythema
answer
Acne Rosacea (Findings include facial erythema, telangiectasias, papules, and pustules. *Does not present with comedomes.* Rosacea is exacerbated by sun exposure, ethanol, and "flushing" agents.)
question
usually in males with long history of sun exposure and ethanol consumption
answer
Rhinophyma (This is a complication of rosacea. Ocular symptoms include blepharitis, conjunctivitis, keratitis.)
question
pustules on acne patient
answer
Gram Negative Folliculitis (Treat with ampicillin or augmentin.)
question
")
*honey crusts* can have vesicles or bullae
answer
Impetigo (Caused by S. aureus or Streptococcus pyogenes.)
question
")
beefy red eroded plaque, intertriginous areas *satellite pustules and papules*
answer
Satellite Candida (Associated with obesity and DM.)
question
beefy red plaque, intertriginous areas *satellite pustules and papules*
answer
Satellite Candida (Associated with obesity and DM.)
question
*lake of pus* with skin sloughing
answer
Pustular Psoriasis (Most commonly limited to palms and soles. Treat with MTX or Soriatane.)
question

Type of acne? A. Comedonal B. Inflammatory C. Mixed D. Nodulocystic E. Rosacea
answer
A. Comedonal
question
white, well demarcated plaque of induration with rim of hyperpigmentation perhaps some violaceous change
answer
Morphea (Biopsy shows markedly thickened collagen bundles, with entrapment or compression of sweat glands, adnexal structures, and blood vessels. *Labs results are negative for ANA, anti-centromere, and Scl-70.*)
question
*coup de sabre*
answer
Morphea (Biopsy shows markedly thickened collagen bundles, with entrapment or compression of sweat glands, adnexal structures, and blood vessels. *Labs results are negative for ANA, anti-centromere, and Scl-70.*)
question
shiny, swollen fingers difficulty opening mouth (beaked facies)
answer
Progressive Systemic Sclerosis (*Positive for ANA, Scl-70. Treat with physical therapy.* Complications include severe HTN, conduction defects, pericarditis, CHF, renal failure, pulmonary fibrosis; esophageal dysmotility and strictures.)
question
")
superficial dilated blood vessels
answer
CREST Syndrome: Telangiectasias (Calcinosis of skin, Raynaud's, Esophageal dysmotility, Sclerodactaly, Telangiectasias; *positive for ANA, anti-centromere, negative for Scl-70.*)
question
")
sausage digits, swollen, shiny
answer
CREST Syndrome: Raynaud's (Calcinosis of skin, Raynaud's, Esophageal dysmotility, Sclerodactaly, Telangiectasias; *positive for ANA, anti-centromere, negative for Scl-70.*)
question
 (Commonly misdiagnosed as child abuse. Treat with high potency topical steroids with or without minocyclin/doxycycline.)")
porcelain white; sharply demarcated with purpura; *cigarette paper* skin usually seen in genital area, but may be generalized
answer
Lichen Sclerosus (et atrophicus) (Commonly misdiagnosed as child abuse. Treat with high potency topical steroids with or without minocyclin/doxycycline.)
question
annular papules/plaques with central clearing seen on the dorsal hands and feet
answer
Granuloma Annulare (Commonly diagnosed as *ringworm, which displays annular papules/plaques with scaling.*)
question

red-brown to yellow plaques with prominent telangiectasias commonly seen on the shins
answer
Necrobiosis Lipoidica (Called "diabeticorum," as 2/3 of patients also have abnormal glucose metabolism.)
question

What is the diagnosis? A. Granuloma annulare B. Morphea C. Necrobiosis lipoidica D. Lichen sclerosus E. Systemic sclerosis
answer
B. Morphea ("coup de sabre*)
question
pinpoint to 3mm in size
answer
Petechiae (Most prominent in legs; if patient is bedridden, in back and sacrum.)
question

ecchymoses; skin atrophy and bleeding usually seen on dorsolateral arms and dorsal hands
answer
Actinic ("Solar") Purpura (Chronic sun induces blood vessel fragility; loss of "shock absorbers" of the dermis. Skin atrophy and solar elastosis is usually severe.)
question
eyelid purpura
answer
Systemic Amyloidosis (Also shows pinch purpura and macroglossia.)
question
petechiae, purpuric stellate (irregular) ecchymosis; central necrosis most characteristic
answer
DIC (Uncontrolled clotting causes diffuse thrombus formation, which leads to consumption of platelets and thrombocytopenia. Other findings include prolonged prothrombin time, hypofibrinogenemia, and fibrinogen degradation products.)
question
palpable purpura of the legs
answer
Leukocytoclastic Cutaneous Vasculitis (Check for fever and arthritis in order to rule out sepsis. Causes include SLE and RA. Order ANA, viral hepatitis panel [especially for Hepatitis C] and rheumatoid factor to determine cause.)
question
")
necrotic, hemorrhagic pustule on extremity may also present with swollen knee
answer
Gonococcemia caused by N. gonorrhoeae (Culture cervical/penile urethra, oropharynx, and rectum; treat with IV ceftriaxone.)
question
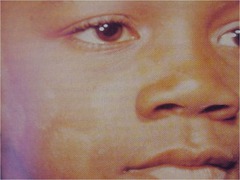
fairly well demarcated, hypopigmented atrophic plaques with fine scale usually seen on chest, back, and shoulders
answer
Tinea (Pityriasis) Versicolor (*Worse in hot/humid environments.*)
question
fairly well demarcated, hyperpigmented atrophic plaques with fine scale usually seen on chest, back, and shoulders
answer
Tinea (Pityriasis) Versicolor (*Worse in hot/humid environments.*)
question
fairly well demarcated, erythematous atrophic plaques with fine scale usually seen on chest, back, and shoulders
answer
Tinea (Pityriasis) Versicolor (*Worse in hot/humid environments.*)
question
*chopped spaghetti and meatballs* KOH stain
answer
Tinea (Pityriasis) Versicolor (Hyphae and spores can be seen.)
question
periorificial, sharply marginated white (depigmented) non-scaly patches
answer
Vitiligo (Associated with Grave's disease and autoimmune thyroiditis, pernicious anemia, alopecia areata, and Addison's disease.)
question
periorificial, sharply marginated white (depigmented) non-scaly patches
answer
Vitiligo (Associated with Grave's disease and autoimmune thyroiditis, pernicious anemia, alopecia areata, and Addison's disease.)
question
process from hair follicle outward
answer
Repigmentation in Vitiligo (Vitiligo is associated with Grave's disease and autoimmune thyroiditis, pernicious anemia, alopecia areata, and Addison's disease.)
question
 1 year.)" alt="Pityriasis Alba (Usually first noticed in spring or summer. Repigmentation takes >1 year.)">
1 year.)" alt="Pityriasis Alba (Usually first noticed in spring or summer. Repigmentation takes >1 year.)">
hypopigmented poorly demarcated atrophic plaques with fine white scale. usually affects the cheeks; also commonly involves upper outer arms
1 year.)" alt="Pityriasis Alba (Usually first noticed in spring or summer. Repigmentation takes >1 year.)">
answer
Pityriasis Alba (Usually first noticed in spring or summer. Repigmentation takes >1 year.)
question
rim of hyperpigmentation at edge scarring in center
answer
Postinflammatory Hypopigmentation (Can be caused by contact dermatitis, autoimmune effects, local trauma; Xrays and frostbite; phenols and sulfhydryl compounds, discoid lupus erythematosus, atopic dermatitis, psoriasis.)
question
subtle, somewhat well-demarcated scaly white patches/macules
answer
Postinflammatory Hypopigmentation (Can be caused by contact dermatitis, autoimmune effects, local trauma; Xrays and frostbite; phenols and sulfhydryl compounds, discoid lupus erythematosus, atopic dermatitis, psoriasis.)
question

"ash-leaf" macule/patch
answer
Tuberous Sclerosis (Cutaneous findings include *ash leaf macules/patches*: 80-90%, *adenoma sebacum*/facial angiofibromas): 80-90%; periungual fibromas/*Koenen's tumors*: 50% *shagreen patches*: 21-80%; flesh to yellowish-orange plaques (*orange peel/pigskin*) usually in the lumbosacral area. Other findings include calcified brain "tubers," mental retardation, seizure disorders, brain tumors, renal cysts, cardiac rhabdomyomas.) )
question
4+ ash-leaf patches
answer
Tuberous Sclerosis (Cutaneous findings include *ash leaf macules/patches*: 80-90%, *adenoma sebacum*/facial angiofibromas): 80-90%; periungual fibromas/*Koenen's tumors*: 50% *shagreen patches*: 21-80%; flesh to yellowish-orange plaques (*orange peel/pigskin*) usually in the lumbosacral area. Other findings include calcified brain "tubers," mental retardation, seizure disorders, brain tumors, renal cysts, cardiac rhabdomyomas.)
question
Shagreen patch "ash-leaf" patch
answer
Tuberous Sclerosis (Cutaneous findings include *ash leaf macules/patches*: 80-90%, *adenoma sebacum*/facial angiofibromas): 80-90%; periungual fibromas/*Koenen's tumors*: 50% *shagreen patches*: 21-80%; flesh to yellowish-orange plaques (*orange peel/pigskin*) usually in the lumbosacral area. Other findings include calcified brain "tubers," mental retardation, seizure disorders, brain tumors, renal cysts, cardiac rhabdomyomas.)
question
adenoma sebaceum angiofibromas dental enamel pits
answer
Tuberous Sclerosis (Cutaneous findings include *ash leaf macules/patches*: 80-90%, *adenoma sebacum*/facial angiofibromas): 80-90%; periungual fibromas/*Koenen's tumors*: 50% *shagreen patches*: 21-80%; flesh to yellowish-orange plaques (*orange peel/pigskin*) usually in the lumbosacral area. Other findings include calcified brain "tubers," mental retardation, seizure disorders, brain tumors, renal cysts, cardiac rhabdomyomas.)
question
Koenen's tumors
answer
Tuberous Sclerosis (Cutaneous findings include *ash leaf macules/patches*: 80-90%, *adenoma sebacum*/facial angiofibromas): 80-90%; periungual fibromas/*Koenen's tumors*: 50% *shagreen patches*: 21-80%; flesh to yellowish-orange plaques (*orange peel/pigskin*) usually in the lumbosacral area. Other findings include calcified brain "tubers," mental retardation, seizure disorders, brain tumors, renal cysts, cardiac rhabdomyomas.)
question

What is the best diagnosis? A. ITP B. Leukocytoclastic vasculitis C. Neisseria infection D. Solar purpura E. TTP
answer
C. Neisseria infection Gonococcemia is the diagnosis; culture cervical/penile urethra, oropharynx, and rectum; treat with IV ceftriaxone.
question
macules, "sprinkled confetti" seen on shins of females
answer
Idiopathic Guttate Hypomelanosis (No good therapy.)
question
")
hypopigmented, hypestetic macule/patch/plaque
answer
Leprosy (Tissue biopsy for Fite stain. Caused by Mycobacterium leprae and spread by armadillos.)
question
")
hypopigmented areas, bathing trunk distribution
answer
Hypopigmented Mycosis Fungoides (Cutaneous T-Cell Lymphoma.)
question
Which of the following may be found in this patient? A. Cafe au lait macules B. Coup de sabre C. Neurofibromas D. Shagreen patch
answer
D. Shagreen patch Cutaneous findings in Tuberous Sclerosis include ash leaf macules/patches: 80-90%, adenoma sebacum/facial angiofibromas): 80-90%; periungual fibromas/Koenen's tumors: 50% shagreen patches: 21-80%; flesh to yellowish-orange plaques (orange peel/pigskin) usually in the lumbosacral area.
question
significant thinning of the parietal region no inflammation or scarring
answer
Telogen Effluvium (Pull test: many telogen hairs (small bulb at end of hair), club-shaped hairs. Order CBC, ANA, RPR, thyroid to rule out anemia, hypothyroidism, nutritional, toxic drugs, lupus, syphilis.)
question
thinning of the vertex scalp
answer
Telogen Effluvium (Pull test: many telogen hairs (small bulb at end of hair), club-shaped hairs. Order CBC, ANA, RPR, thyroid to rule out anemia, hypothyroidism, nutritional, toxic drugs, lupus, syphilis.)
question
no scarring or inflammation
answer
Androgenic Alopecia (Caused by a testosterone-induced reversion of mature hair to vellus hairs in a specific pattern; physical exam shows nonscarring, frontal, vertex affected terminal hairs replaced by vellus, smooth shiny scalp; will see diffuse thinning of vertex in women.)
question
no scarring or inflammation
answer
Androgenic Alopecia (Caused by a testosterone-induced reversion of mature hair to vellus hairs in a specific pattern; physical exam shows nonscarring, frontal, vertex affected terminal hairs replaced by vellus, smooth shiny scalp; will see diffuse thinning of vertex in women.)
question
vertex loss
answer
Androgenic Alopecia (Caused by a testosterone-induced reversion of mature hair to vellus hairs in a specific pattern; physical exam shows nonscarring, frontal, vertex affected terminal hairs replaced by vellus, smooth shiny scalp; will see diffuse thinning of vertex in women.)
question
irregularly-shaped with variable hair length no scaling or erythema
answer
Trichotillomania (Caused by self-induced traumatic hair loss by plucking, twisting or rubbing; physical exam shows empty hair follicles in *strange geometric patterns*, traumatized follicles, perifollicular hemorrhage, pigmentary casts, increased number of catagen hairs.)
question
diffuse thinning "difficult to tell here"
answer
Trichotillomania (Caused by self-induced traumatic hair loss by plucking, twisting or rubbing; physical exam shows empty hair follicles in *strange geometric patterns*, traumatized follicles, perifollicular hemorrhage, pigmentary casts, increased number of catagen hairs.)
question
bizarre geometric shape
answer
Trichotillomania (Caused by self-induced traumatic hair loss by plucking, twisting or rubbing; physical exam shows empty hair follicles in *strange geometric patterns*, traumatized follicles, perifollicular hemorrhage, pigmentary casts, increased number of catagen hairs.)
question
oval/round patch, exclamation point hairs
answer
Alopecia Areata (Caused by autoimmune hair loss; physical exam shows *round or oval patches, exclamation point hairs*, no inflammation or scarring and skin biopsy shows *"Swarm of Bees"*- lymphocytes surrounding base of hair follicles.)
question
sharply demarcated, oval and smooth patch
answer
Alopecia Areata, Ophiasis type (most common) (Caused by autoimmune hair loss; physical exam shows *round or oval patches, exclamation point hairs*, no inflammation or scarring and skin biopsy shows *"Swarm of Bees"*- lymphocytes surrounding base of hair follicles.)
question
totalis
answer
Alopecia Areata (Caused by autoimmune hair loss; physical exam shows *round or oval patches, exclamation point hairs*, no inflammation or scarring and skin biopsy shows *"Swarm of Bees"*- lymphocytes surrounding base of hair follicles.)
question

answer
Nonspecific nail pitting, here associated with Alopecia Areata
question
erythema scaling some scarring, possibly
answer
Lupus Erythematosus (Causes chronic/discoid patchy scarring or non-scarring alopecia; broken hairs at frontal hairline, carpet tack scale, dyspigmentation, inflammation. Biopsy shows interface dermatitis- lymphocytic infiltrate and DE junction, liquifactive degeneration of basal cells, follicular plugging.)
question
lots of erythema scaling
answer
Lupus Erythematosus (Causes chronic/discoid patchy scarring or non-scarring alopecia; broken hairs at frontal hairline, carpet tack scale, dyspigmentation, inflammation. Biopsy shows interface dermatitis- lymphocytic infiltrate and DE junction, liquifactive degeneration of basal cells, follicular plugging.)
question
young children
answer
Tinea Capitis (Demonstrates scarring alopecia [*if you see scarring on the scalp of a child, think tinea*]; useful labs include Wood's light, KOH exam, culture; griseofulvin is the gold standard of treatment; *topicals do not work.*)
question
exclamation point young child
answer
Tinea Capitis (Demonstrates scarring alopecia [*if you see scarring on the scalp of a child, think tinea*]; useful labs include Wood's light, KOH exam, culture; griseofulvin is the gold standard of treatment; *topicals do not work.*)
question
Diagnosis in this 8 year old? A. Exzema B. Discoid Lupus erythematous C. Psoriasis D. Seborrheic Dermatitis E. Tinea capitis
answer
E. Tinea capitis (Demonstrates scarring alopecia [*if you see scarring on the scalp of a child, think tinea*]; useful labs include Wood's light, KOH exam, culture; griseofulvin is the gold standard of treatment; *topicals do not work.*)
question
")
"crumbly nails" debris, yellow change DIFFERENTIAL psoriasis, trauma, lichen planus
answer
Onychomycosis (Most commonly caused by T. rubrum, T. mentagrophytes; physical exam shows yellow, thickening and dystrophy, subungual debris, superficial white changes.)
question
hallux involvement
answer
Onychomycosis (Most commonly caused by T. rubrum, T. mentagrophytes; physical exam shows yellow, thickening and dystrophy, subungual debris, superficial white changes.)
question

onycholysis oil drop
answer
Psoriasis (Caused by increased rate of proliferation of keratinocytes; physical exam shows *nail pitting*, dystrophy, onycholysis, *"oil drop sign"* [yellow color under nail], fingernails affected more than toenails.)
question
pitting
answer
Psoriasis (Caused by increased rate of proliferation of keratinocytes; physical exam shows *nail pitting*, dystrophy, onycholysis, *"oil drop sign"* [yellow color under nail], fingernails affected more than toenails.)
question
nail and skin involvement pustules, "lakes of pus"
answer
Pustular Psoriasis (Most commonly limited to palms and soles. Treat with MTX or Soriatane.)
question
answer
Psoriasis (Caused by increased rate of proliferation of keratinocytes; physical exam shows *nail pitting*, dystrophy, onycholysis, *"oil drop sign"* [yellow color under nail], fingernails affected more than toenails.)
question
red, swollen
answer
Acute Paronychia (ACUTE S. aureus infection leading to inflammation and infection of proximal and lateral nail folds; red, swollen, painful; CHRONIC Candida infection leading to inflammation and infection of proximal and lateral nail folds; loss of cuticle, creases in nail plate, scaling)
question
swollen
answer
Acute Paronychia (ACUTE S. aureus infection leading to inflammation and infection of proximal and lateral nail folds; red, swollen, painful; CHRONIC Candida infection leading to inflammation and infection of proximal and lateral nail folds; loss of cuticle, creases in nail plate, scaling)
question
180 degrees)" alt="Clubbing (Bulbous thickening of distal digit, proximal nail fold soft and thickened; hypertrophic osteoarthropathy; Lovibond's angle > 180 degrees)">
answer
Clubbing (Bulbous thickening of distal digit, proximal nail fold soft and thickened; hypertrophic osteoarthropathy; Lovibond's angle > 180 degrees)
question
spoon-shaped
answer
Koilonychia (Caused by iron deficiency anemia, Plummer-Vinson syndrome, Hemachromatosis, CAD, syphilis, polycythemia, acanthosis nigricans, familial forms; physical exam shows spoon nails, thin and concave)
question
transverse furrows affecting all nails
answer
Beau's Lines (Temporary arrest of growth of nail plate leading to ransverse furrows that grow out; Triggered by traumatic/stressful events: childbirth, febrile illness, drug reaction. Note that the nails *grow out at a rate of 1mm/month.*)
question
What is the diagnosis? A. Beau's lines B. Clubbing C. Fungus D. Koilonychia E. Paronychia F. Psoriasis
answer
A. Beau's Lines (Temporary arrest of growth of nail plate leading to ransverse furrows that grow out; Triggered by traumatic/stressful events: childbirth, febrile illness, drug reaction. Note that the nails *grow out at a rate of 1mm/month.*)
question
medial aspect of lower leg full thickness epidermal loss with petechiae (pinpoint - 3 mm)
answer
Stasis (Venous Insufficiency) Ulcers (Common in CHF and incompetent leg vein vales; physical exam shows significant, bilateral swelling of medial lower legs, brownish dyspigmentation and petechiae, commonly *Most common etiology of leg ulcers,* check DP/PT pulses to rule out associated arterial disease.)
question
sharply demarcated, "punched out" ulcer
answer
Arterial Ulcers (History commonly shows intermittent claudication, rest pain; physical exam demonstrates punched out ulcers on the lateral aspects of the legs (classically); DP/PT pulses absent, cool extremities, local hair loss.)
question
cribriform scarring
answer
Pyoderma Grangrenosum (Physical exam shows distinctive ulceration: acute onset of a painful ulcer with an undermined border [Dr. Stetson likes to say "you could stick a probe into it"], which heals with *cribriform scarring*; associated with ulcerative colitis, rheumatoid arthritis, and acute myeloblastic leukemia; *biopsy reveals neutrophils throughout the dermis, but cultures are negative.*)
question
")
answer
Chancre in Primary Syphilis (Note that the *chancre caused by Treponema pallidum is painless*, whereas the *chancroid caused by Haemophilus ducreyi is painful*.)
question
")
dark field microscopy
answer
Spirochetes (You can test for the syphilitic Treponema pallidum by dark field microscopy.)
question
")
*"nickles and dimes" on palm*
answer
Secondary Syphilis HIGHLY STRESSED)
question
"moth-eaten" alopecia
answer
Secondary Syphilis
question
")
"punched out, painful" ulcers
answer
Chancroid (This is caused by Haemophilus ducreyi, and should be differentiated from the chancre of primary syphilis, as caused by Treponema pallidum.)
question
painful, ragged ulcer "undetermined" NOTE difficult to culture
answer
Chancroid (This is caused by Haemophilus ducreyi, and should be differentiated from the chancre of primary syphilis, as caused by Treponema pallidum.)
question
"school of fish" gram negative coccobacilli
answer
Haemophilis ducreyi (Causative agent of chancroid.)
question

grouped ulcerations on erythematous base
answer
HSV
question
grouped vesicles on erythematous base
answer
HSV
question
Tzanck smear showing multinucleated keratinocytes, ballooning degeneration steel-gray nuclei chromatin margination
answer
HSV
question
*angulated linear heme-crusted ulcer*
answer
Factitial Ulcer (Causes include a variety of insults: deep excoriations, injections of foreign material, heat/cold. Note that the patient will often deny causing the ulceration and the history will be unreliable. These ulcers appear as bizarre, geometric shaped angulated ulcers. Must be suspected clinically; especially if location is unusual for ulcerations, and there are no other explanation for the ulcer.)
question

What is the best diagnosis? A. Arterial ulcer B. Factitial ulcer C. Pyoderma gangrenosum D. Stasis ulcer E. Syphilis
answer
C. Pyoderma gangrenosum Note underlying edge, where "one could stick a probe."
question
cheek, arms
answer
Eczema, Atopic Dermatitis (Most common form is atopic dermatitis; appearance is classically more ill-defined scaly erythematous coalescing papules and plaques; *infantile form favors face*, scalp and extensors; 80% develop allergic rhinitis)
question
plaque, erythematous papules seborrheic appearance
answer
Eczema, Atopic Dermatitis (Appearance is classically more ill-defined scaly erythematous coalescing papules and plaques; *childhood form favors flexors; often lichenified*; 40% have persistent disease as adults)
question
")
possible lichenification in the cubital fossa
answer
Eczema (Appearance is classically more ill-defined scaly erythematous coalescing papules and plaques; *childhood form favors flexors; often lichenified*; 40% have persistent disease as adults)
question
hyperlinear palms
answer
Eczema (Associated with keratosis pilaris, xerosis, icthyosis vulgaris, Dennie-morgan lines, *hyperlinear palms*, pityriasis alba; can become erythrodermic. Often impetiginized [S. aureus, honey crusted] or considered *eczema herpeticum [painful super-infection by HSV]*).
question
")
thickening NOTE the papulovesicles on the lateral finger
answer
Hand Dermatitis (Caused by contact irritant or allergy; can also be associated with foot/ feet dermatitis; related to atopic dermatitis)
question
answer
Hand Dermatitis (Caused by contact irritant or allergy; can also be associated with foot/ feet dermatitis; related to atopic dermatitis)
question
answer
Hand Dermatitis (Caused by contact irritant or allergy; can also be associated with foot/ feet dermatitis; related to atopic dermatitis)
question

"plate-like or fish-like" changes dry river bed
answer
Asteatotic Eczema (Appearance is termed "eczema craquele" and "dried river bed;" favors shins, flanks, post axillary line. Associated with aging, xerosis, low humidity, frequent bathing)
question
*coin-shaped*, scaly
answer
Nummular Dermatitis (Appears as pruritic coin-shaped eczematous lesions with a chronic, recurrent course. Associated with contact sensitization and stasis, but not atopy. More common in older patients.)
question
answer
Nummular Dermatitis (Appears as pruritic coin-shaped eczematous lesions with a chronic, recurrent course. Associated with contact sensitization and stasis, but not atopy. More common in older patients.)
question
eye involvement linear pattern
answer
Phyto Contact Dermatitis (Poison Ivy here) (Usually eczematous in appearance; caused by irritants in 80% of cases and by allergies in 20% of cases [this includes application of *Neosporin/Polysporin/Triple antibiotics or topical benadryl*])
question
eczematous changes with vesicles
answer
Acute Contact Dermatitis (Usually eczematous in appearance; caused by irritants in 80% of cases and by allergies in 20% of cases [this includes application of *Neosporin/Polysporin/Triple antibiotics or topical benadryl*])
question
answer
Contact Dermatitis, caused by leather (Usually eczematous in appearance; caused by irritants in 80% of cases and by allergies in 20% of cases [this includes application of *Neosporin/Polysporin/Triple antibiotics or topical benadryl*])
question
![Seborrheic Dermatitis (Favors scalp, ears, face, central chest, and intertrigious areas; associated with with Malassezia Furfur [pitrysorom ovale]; can be severe and refractory in HIV)](https://studyhippo.com/wp-content/uploads/2018/04/seborrheic-dermatitisfavors-scalp-ears-face-central-chest-and-intertrigious-areas-associated-with-with-malassezia-furfur-pitrysorom-ovalecan-be-severe-and-refractory-in-hiv.jpg "Seborrheic Dermatitis (Favors scalp, ears, face, central chest, and intertrigious areas; associated with with Malassezia Furfur [pitrysorom ovale]; can be severe and refractory in HIV)")
scalp involvement
answer
Seborrheic Dermatitis (Favors scalp, ears, face, central chest, and intertrigious areas; associated with with Malassezia Furfur [pitrysorom ovale]; can be severe and refractory in HIV)
question
intertrigious area
answer
Seborrheic Dermatitis, here as cradle cap in infant (Favors scalp, ears, face, central chest, and intertrigious areas; associated with with Malassezia Furfur [pitrysorom ovale]; can be severe and refractory in HIV)
question
eyebrow scaling
answer
Seborrheic Dermatitis (Favors scalp, ears, face, central chest, and intertrigious areas; associated with with Malassezia Furfur [pitrysorom ovale]; can be severe and refractory in HIV)
question
scalp and forehead involvement
answer
Seborrheic Dermatitis (Favors scalp, ears, face, central chest, and intertrigious areas; associated with with Malassezia Furfur [pitrysorom ovale]; can be severe and refractory in HIV)
question
brown, angular, ring shaped could be fungal
answer
Seborrheic Dermatitis (Favors scalp, ears, face, central chest, and intertrigious areas; associated with with Malassezia Furfur [pitrysorom ovale]; can be severe and refractory in HIV)
question
impressive scaling and redness over the face guttate (drop-like)
answer
Seborrheic Dermatitis (Favors scalp, ears, face, central chest, and intertrigious areas; associated with with Malassezia Furfur [pitrysorom ovale]; can be severe and refractory in HIV)
question
answer
Seborrheic Dermatitis (Favors scalp, ears, face, central chest, and intertrigious areas; associated with with Malassezia Furfur [pitrysorom ovale]; can be severe and refractory in HIV)
question
varicosities, venous ulceration pigmentary changes
answer
Stasis Dermatitis (Appears as eczematous dermatitis due to venous insufficiency and dependent edema; often associated with allergic contact dermatitis. Stasis dermatitis is often seen in combination with venous hypertension, varicosities, edema, venous ulceration, hemosiderin deposits, and lipodermatosclerosis, and confers a risk for stasis ulcer and contact sensitization/ dermatitis)
question
petechiae, ulceration, hyperpigmentation
answer
Stasis Dermatitis (Appears as eczematous dermatitis due to venous insufficiency and dependent edema; often associated with allergic contact dermatitis. Stasis dermatitis is often seen in combination with venous hypertension, varicosities, edema, venous ulceration, hemosiderin deposits, and lipodermatosclerosis, and confers a risk for stasis ulcer and contact sensitization/ dermatitis)
question
pigmentary changes only, longstanding
answer
Stasis Dermatitis (Appears as eczematous dermatitis due to venous insufficiency and dependent edema; often associated with allergic contact dermatitis. Stasis dermatitis is often seen in combination with venous hypertension, varicosities, edema, venous ulceration, hemosiderin deposits, and lipodermatosclerosis, and confers a risk for stasis ulcer and contact sensitization/ dermatitis)
question
answer
Lichen Simplex Chronicus (Secondary finding due to chronic rubbing and scratching; continued by *Itch-scratch-itch cycle*)
question
spikiness; not all at same level vertical streaking of collagen *irregular epithelial hyperplasia* NOTE compare to psoriasis histology
answer
Lichen Simplex Chronicus (Secondary finding due to chronic rubbing and scratching; continued by *Itch-scratch-itch cycle*)
question
![Neurodermatitis (Neurodermatitis/Neurodermatology includes delusions of parasitosis, factitional disorders, and endogenous pruritus [kidney, liver, thyroid, anemia, lymphoma, parasites, other])](https://studyhippo.com/wp-content/uploads/2018/04/neurodermatitisneurodermatitis-neurodermatology-includes-delusions-of-parasitosis-factitional-disorders-and-endogenous-pruritus-kidney-liver-thyroid-anemia-lymphoma-parasites-other.jpg "Neurodermatitis (Neurodermatitis/Neurodermatology includes delusions of parasitosis, factitional disorders, and endogenous pruritus [kidney, liver, thyroid, anemia, lymphoma, parasites, other])")
irregular presentation linear heme crusts post inflammatory changes
answer
Neurodermatitis (Neurodermatitis/Neurodermatology includes delusions of parasitosis, factitional disorders, and endogenous pruritus [kidney, liver, thyroid, anemia, lymphoma, parasites, other])
question
old scarring from past flares angulated upper back only
answer
Neurodermatitis (Neurodermatitis/Neurodermatology includes delusions of parasitosis, factitional disorders, and endogenous pruritus [kidney, liver, thyroid, anemia, lymphoma, parasites, other])
question
linear scratches DIFFERENTIAL contact dermatitis
answer
Neurodermatitis (Neurodermatitis/Neurodermatology includes delusions of parasitosis, factitional disorders, and endogenous pruritus [kidney, liver, thyroid, anemia, lymphoma, parasites, other])
question
bizarre ulceration pattern
answer
Neurodermatitis (Neurodermatitis/Neurodermatology includes delusions of parasitosis, factitional disorders, and endogenous pruritus [kidney, liver, thyroid, anemia, lymphoma, parasites, other])
question
sharply demarcated, erythematous papules, plaques, some annular (central clearing) not very much scaling truncal predominance
answer
Pityraisis Rosea (Appears as *classically well circumscribed papules and plaques* in a "Christmas" or "fir" tree appearance on back, upside down on chest; primarily involves trunk. The primary plaque is referred to as a herald patch.)
question
sharply demarcated annular and erythematous papules and plaques truncal distribution
answer
Pityriasis Rosea (Appears as *classically well circumscribed papules and plaques* in a "Christmas" or "fir" tree appearance on back, upside down on chest; primarily involves trunk. The primary plaque is referred to as a herald patch.)
question
papulosquamous eruption at scalp thick scaling
answer
Psoriasis (Appearance is a classic papulosquamous eruption favoring elbows, knees, scalp, and sacral area, *usually sparing the face*. Nail findings [onycholysis, pits, oil drop (most specific] are highly correlated with arthritis.)
question
papulosquamous eruption sharply demarcated scaly
answer
Psoriasis (Appearance is a classic papulosquamous eruption favoring elbows, knees, scalp, and sacral area, *usually sparing the face*. Nail findings [onycholysis, pits, oil drop (most specific] are highly correlated with arthritis.)
question
very erythematous swollen joints with potential arthritic changes
answer
Psoriasis (Appearance is a classic papulosquamous eruption favoring elbows, knees, scalp, and sacral area, *usually sparing the face*. Nail findings [onycholysis, pits, oil drop (most specific] are highly correlated with arthritis.)
question
*nail pitting* plaque on right
answer
Psoriasis (Appearance is a classic papulosquamous eruption favoring elbows, knees, scalp, and sacral area, *usually sparing the face*. Nail findings [onycholysis, pits, oil drop (most specific] are highly correlated with arthritis.)
question
onycholysis *oil drop*
answer
Psoriasis (Appearance is a classic papulosquamous eruption favoring elbows, knees, scalp, and sacral area, *usually sparing the face*. Nail findings [onycholysis, pits, oil drop (most specific] are highly correlated with arthritis.)
question
club shaped equal level NOTE compare to histology of lichen simplex chronicus
answer
Psoriasis (Dermatologic appearance is a classic papulosquamous eruption favoring elbows, knees, scalp, and sacral area, *usually sparing the face*. Nail findings [onycholysis, pits, oil drop (most specific] are highly correlated with arthritis.)
question
*Monroe's microabscess* NOTE compare to histology of lichen simplex chronicus
answer
Psoriasis (Appearance is a classic papulosquamous eruption favoring elbows, knees, scalp, and sacral area, *usually sparing the face*. Nail findings [onycholysis, pits, oil drop (most specific] are highly correlated with arthritis.)
question
plaques, slightly scaly buttocks and lower trunk most affected
answer
Mycosis Fungoides, a cutaneous T cell lymphoma (Erythrodermic patch progresses to intensely pruritic, well-developed plaques in a *bathing trunk distribution* [clinically diagnostic]. These then progress to low grade, insidious tumors. Less developed lesions are typically not pruritic. Median duration from onset to definitive diagnosis is 4-6 years. Dermatopathic lymphadenopathy usually present.)
question
orange/salmon color some scaling
answer
Mycosis Fungoides, a cutaneous T cell lymphoma (Erythrodermic patch progresses to intensely pruritic, well-developed plaques in a *bathing trunk distribution* [clinically diagnostic]. These then progress to low grade, insidious tumors. Less developed lesions are typically not pruritic. Median duration from onset to definitive diagnosis is 4-6 years. Dermatopathic lymphadenopathy usually present.)
question

answer
Tinea (Use "capitis" for scalp, "manum" for hand, "pedis" for foot, "cruris" for groin area, "ungium" for nail, "corporis" for body- location 'not otherwise specified'.)
question

annulare with scaling
answer
Tinea (Use "capitis" for scalp, "manum" for hand, "pedis" for foot, "cruris" for groin area, "ungium" for nail, "corporis" for body- location 'not otherwise specified'.)
question
answer
Tinea (Use "capitis" for scalp, "manum" for hand, "pedis" for foot, "cruris" for groin area, "ungium" for nail, "corporis" for body- location 'not otherwise specified'.)
question
answer
Tinea (Use "capitis" for scalp, "manum" for hand, "pedis" for foot, "cruris" for groin area, "ungium" for nail, "corporis" for body- location 'not otherwise specified'.)
question
answer
Tinea (Use "capitis" for scalp, "manum" for hand, "pedis" for foot, "cruris" for groin area, "ungium" for nail, "corporis" for body- location 'not otherwise specified'.)
question
segmented; hyphae in fungus
answer
Tinea (Use "capitis" for scalp, "manum" for hand, "pedis" for foot, "cruris" for groin area, "ungium" for nail, "corporis" for body- location 'not otherwise specified'.)
question
What is the most likely diagnosis? A. Allergic contact dermatitis B. Candidiasis C. Eczema D. Psoriasis E. Tinea
<img src="https://chmanchacentro.com/wp-content/uploads/2018/04/c-eczemanote-that-this-is-on-the-cheek-in-a-child-approximately.jpg" title="C. Eczema Note that this is on the cheek in a child approximately <2 months. Psoriasis does not "like" the face. (Most common form of eczema is atopic dermatitis; appearance is classically more ill-defined scaly erythematous coalescing papules and plaques; *infantile form favors face*, scalp and extensors; 80% develop allergic rhinitis)" alt="C. Eczema Note that this is on the cheek in a child approximately
answer
C. Eczema Note that this is on the cheek in a child approximately <2 months. Psoriasis does not "like" the face. (Most common form of eczema is atopic dermatitis; appearance is classically more ill-defined scaly erythematous coalescing papules and plaques; *infantile form favors face*, scalp and extensors; 80% develop allergic rhinitis)
question
round, "punched out" ulcers yellow/white necrotic base with surrounding erythema
answer
Aphthous Stomatitis (Affects 20-60% of the population and manifests as recurrent, idiopathic oral ulcers commonly called "canker sores" with a whitish, yellow necrotic surface/base and surrounding erythema; variants include herpetiform and major aphthae [1-3 cm; may be an initial manifestation of Behcet's, but this is rare in Lubbock].)
question
uncommon oral ulcer
answer
Histoplasmosis
question
")
uncommon oral ulcer
answer
Pemphigus Vulgaris (90% will develop oral ulcers, and 50% present with oral ulcers, may involve buccal mucosa or tongue.)
question
uncommon ulcerative scarring of mucosa
answer
Mucosal/Cicatricial Pemphigoid
question
blister on erythematous base
answer
Herpes Labialis
question
blisters, erythema around it on hand
answer
Hand, Foot, Mouth Disease (Diagnosis especially likely if dermatologic findings are in a child.)
question

answer
Squamous Cell Carcinoma of the Lip
question

answer
Squamous Cell Carcinoma of the Tongue
question
plaque
answer
Leukoplakia (Appearance is a "white-plaque" that does not scrape off, commonly seen in the middle aged and elderly with history of gradual onset, smoking, snuff, dentures. Biopsy shows hyperkeratosis, acanthosis, dysplasia and atypia, lymphocytic infiltrate, carcinoma in-situ.)
question
plaque
answer
Leukoplakia (Appearance is a "white-plaque" that does not scrape off, commonly seen in the middle aged and elderly with history of gradual onset, smoking, snuff, dentures. Biopsy shows hyperkeratosis, acanthosis, dysplasia and atypia, lymphocytic infiltrate, carcinoma in-situ.)
question
")
histologically appears like psoriasis
answer
Geographic tongue (Occurs after eating hot foods or drinking hot beverages; benign finding that will heal.)
question
What is the best diagnosis? A. Candidiasis B. Cicatricial pemphigoid C. Herpes virus infection D. Pemphigus vulgaris E. Syphilis
answer
C. Herpes virus infection
question
Is this lesion malignant? A. True B. False
answer
A. True Note the pearly color and presence of telangiectasias. This is a basal cell carcinoma.
question
flesh-colores firm papules/nodules interrupts normal skin lines usually on hands, fingers
answer
Verruca Vulgaris, the Common Wart (Caused by multiple types of human papilloma virus infecting epidermal cells. Appears as flesh-colored firm papule or nodule with hyperkeratotic (corrugated) surface with black dots, interrupting normal skin lines. Commonly found on hands, fingers. Treat with *non-specific destruction*.)
question
flesh-colores firm papules/nodules interrupts normal skin lines usually on hands, fingers
answer
Verruca Vulgaris, the Common Wart (Caused by multiple types of human papilloma virus infecting epidermal cells. Appears as flesh-colored firm papule or nodule with hyperkeratotic (corrugated) surface with black dots, interrupting normal skin lines. Commonly found on hands, fingers. Treat with *non-specific destruction*.)
question
Slightly raised, flat surfaced papule
answer
Flat Warts
question

often covered by callus can be painful
answer
Plantar Warts
question
soft, moist papule cauliflower-like
answer
Condyloma Acuminatum, the Venereal Wart (Appears as a soft, moist papule or plaque, can be sessile or pedunculated and is often cauliflower-like.)
question
yellow-brown, well circumscribed, scaly papules not interrupting skin lines usually on feet and toes
answer
Corn (Clavus or Heloma) (Localized thickening of epidermis caused by pressure or friction, appears as white-gray or yellow-brown, well circumscribed, scaly papules or nodules that *do not interrupt skin lines*; most commonly involving toes. )
question
tan to dark brown; round and waxy *"stuck on"*, like you could peel it off
answer
Seborrheic Keratosis (Arises as benign neoplasm of epidermal cells; appearance varies in size and color: flesh, tan, brown, occasionally black; oval to round, waxy, well-demarcated, *"stuck on"* appearance; may have *verrucous* or crumbly surface, occasionally with keratin-filled pits. Spares palms and soles.)
question
tan to dark brown; round and waxy-appearing *"stuck on"*, like you could peel it off
answer
Seborrheic Keratosis (Arises as benign neoplasm of epidermal cells; appearance varies in size and color: flesh, tan, brown, occasionally black; oval to round, waxy, well-demarcated, *"stuck on"* appearance; may have *verrucous* or crumbly surface, occasionally with keratin-filled pits. Spares palms and soles.)
question
soft, *pedunculated* papule
answer
Skin Tag (An extremely common benign fleshy tumor; appears as a tan- to flesh-colored, soft *pedunculated* papule with smooth, folded surface. Commonly found on the eyelids, neck, and skin folds (inframammary, axilla, inguinal). No therapy is necessary.)
question
flesh-colored papules with smooth, folded surface in the axilla
answer
Skin Tag (An extremely common benign fleshy tumor; appears as a tan- to flesh-colored, soft *pedunculated* papule with smooth, folded surface. Commonly found on the eyelids, neck, and skin folds (inframammary, axilla, inguinal). No therapy is necessary.)
question
hard, smooth, dome-shaped flesh-colored central *umbilication with "cheesy" core*
answer
Molluscum Contagiosum (Caused by *poxvirus infection* of epidermal cells, common in childhood; also venereal transmission as an adult; *suspect HIV if 100s of persistent lesions*; will commonly see pontaneous *remission* over several months. Appears as 2-5mm hard, smooth, dome-shaped flesh colored or translucent papules demonstrating *central umbilication with 'cheesy' core content*.)
question
hard, smooth, dome-shaped flesh-colored central *umbilication with "cheesy" core*
answer
Molluscum Contagiosum (Caused by *poxvirus infection* of epidermal cells, common in childhood; also venereal transmission as an adult; *suspect HIV if 100s of persistent lesions*; will commonly see pontaneous *remission* over several months. Appears as 2-5mm hard, smooth, dome-shaped flesh colored or translucent papules demonstrating *central umbilication with 'cheesy' core content*.)...
question
rough, yellowish adherent scale
<img src="https://chmanchacentro.com/wp-content/uploads/2018/04/actinic-keratoses-sun-spotsprecancerous-epidermal-neoplasm-caused-by-exposure-to-uv-light-appears-as-1-10-mm-wide-reddish-ill-defined-indistinct-borders-with-rough-yellowish-adherent-scale-o.jpg" title="Actinic Keratoses ("Sun Spots") (Precancerous epidermal neoplasm caused by exposure to UV light. Appears as 1-10-mm wide reddish, ill-defined indistinct borders with rough, yellowish adherent scale. Often easier felt than seen. Small number (~< 1/1000 per year) develop into squamous cell carcinoma.)" alt="Actinic Keratoses ("Sun Spots") (Precancerous epidermal neoplasm caused by exposure to UV light. Appears as 1-10-mm wide reddish, ill-defined indistinct borders with rough, yellowish adherent scale. Often easier felt than seen. Small number (~
answer
Actinic Keratoses ("Sun Spots") (Precancerous epidermal neoplasm caused by exposure to UV light. Appears as 1-10-mm wide reddish, ill-defined indistinct borders with rough, yellowish adherent scale. Often easier felt than seen. Small number (~< 1/1000 per year) develop into squamous cell carcinoma.)
question
rough, yellowish adherent scale
<img src="https://chmanchacentro.com/wp-content/uploads/2018/04/actinic-keratoses-sun-spotsprecancerous-epidermal-neoplasm-caused-by-exposure-to-uv-light-appears-as-1-10-mm-wide-reddish-ill-defined-indistinct-borders-with-rough-yellowish-adherent-scale-o.jpg" title="Actinic Keratoses ("Sun Spots") (Precancerous epidermal neoplasm caused by exposure to UV light. Appears as 1-10-mm wide reddish, ill-defined indistinct borders with rough, yellowish adherent scale. Often easier felt than seen. Small number (~< 1/1000 per year) develop into squamous cell carcinoma.)..." alt="Actinic Keratoses ("Sun Spots") (Precancerous epidermal neoplasm caused by exposure to UV light. Appears as 1-10-mm wide reddish, ill-defined indistinct borders with rough, yellowish adherent scale. Often easier felt than seen. Small number (~
answer
Actinic Keratoses ("Sun Spots") (Precancerous epidermal neoplasm caused by exposure to UV light. Appears as 1-10-mm wide reddish, ill-defined indistinct borders with rough, yellowish adherent scale. Often easier felt than seen. Small number (~< 1/1000 per year) develop into squamous cell carcinoma.)...
question
scaling, indurated nodule
answer
Squamous Cell Carcinoma (Malignancy of *keratinocytes caused by UV light with potential to metastasize* [2% overall], appearing as a scaling, indurated plaque or nodule that sometimes bleeds or ulcerates. Persistent ulceration or bleeding warrants a biopsy. *Treat by surgical excision*)
question
scaling plaque
answer
Squamous Cell Carcinoma (Malignancy of *keratinocytes caused by UV light with potential to metastasize* [2% overall], appearing as a scaling, indurated plaque or nodule that sometimes bleeds or ulcerates. Persistent ulceration or bleeding warrants a biopsy. *Treat by surgical excision*)
question
")
red, scaly, crusted and well-defined plaque
answer
Bowen's Disease (Squamous Cell Carcinoma in Situ)
question
")
rapidly growing, crater-like nodule
answer
Keratoacanthoma (May involute, but difficult to differentiate from SCC, so treat regardless.)
question
pearly, semitranslucent nodules central depression
answer
Basal Cell Carcinoma (Malignancy of the *epidermal basal cell* that rarely metastasizes, but can be *locally destructive*; caused most commonly by *UV radiation*, nodular subtype most common. Appears as a *pearly*, semitranslucent papule or nodule, often with central depression and *telangiectasias*. Borders are rolled and waxy or cratered. *Treat with surgery.*(
question
ulceration and crusting pearly appearance with telangiectasias
answer
Basal Cell Carcinoma with Rodent Ulcer (Malignancy of the *epidermal basal cell* that rarely metastasizes, but can be *locally destructive*; caused most commonly by *UV radiation*. Appears as a *pearly*, semitranslucent papule or nodule, often with central depression and *telangiectasias*. Borders are rolled and waxy or cratered. *Treat with surgery.*)
question

pearly with rolled margin shiny blue-black color, speckled
answer
Pigmented Basal Cell Carcinoma
question
pearly with telangiectasias blue-black color, speckled
answer
Pigmented Basal Cell Carcinoma
question
red, slightly scaling, well-demarcated plaque DIFFERENTIAL eczema
answer
Superficial Basal Cell Carcinoma
question
red, slightly scaling, well-demarcated plaque DIFFERENTIAL eczema
answer
Superficial Basal Cell Carcinoma
question
 Basal Cell Carcinoma (Least common and most aggressive.)")
atrophic white plaque that looks like scar
answer
Sclerosing (Scarring) Basal Cell Carcinoma (Least common and most aggressive.)
question
atrophic white plaque that looks like scar
answer
Sclerosing (Scarring) Basal Cell Carcinoma (Least common and most aggressive.)
question
flesh-colored solitary nodule with central pore
answer
Epidermal Inclusion Cyst / Epidermoid Cyst (Derived from the upper portion of the hair follicle lining and commonly located in the mid and lower dermis. *Discharges cheesy, foul-smelling macerated keratin*. Appears as a flesh-colored, firm, but often malleable, solitary nodule with central punctum or pore. *Multiple epidermal inclusion cysts are a feature of Gardner's syndrome.*)
question
flesh-colored solitary nodule with central pore
answer
Epidermal Inclusion Cyst / Epidermoid Cyst (Derived from the upper portion of the hair follicle lining and commonly located in the mid and lower dermis. *Discharges cheesy, foul-smelling macerated keratin*. Appears as a flesh-colored, firm, but often malleable, solitary nodule with central punctum or pore. *Multiple epidermal inclusion cysts are a feature of Gardner's syndrome.*)
question
bright red lesion
answer
Hemangioma, Superficial (Benign proliferation of blood vessels in dermis and subcutis, most commonly arising in infancy and regressing spontaneously after first year of life; color depends on size and depth of vessels.)
question
bluish lesion
answer
Hemangioma, Subcutaneous (Benign proliferation of blood vessels in dermis and subcutis, most commonly arising in infancy and regressing spontaneously after first year of life; color depends on size and depth of vessels.)
question
bright red, dome-shaped lesion
answer
Hemangioma, Mixed (Benign proliferation of blood vessels in dermis and subcutis, most commonly arising in infancy and regressing spontaneously after first year of life; color depends on size and depth of vessels.)
question
Pinching shows central dimpling Light tan to dark brown
answer
Dermatofibroma (Dermal fibrotic papule or small nodule of unknown origin, possibly trauma; appears as a slightly elevated area ~5mm, often with overlying hyperpigmentation and epidermal thickening. When palpated, these are firm and indurated; demonstrate *"dimple sign."*)
question
dark brown, overlying hyperpigmentation and thickening
answer
Dermatofibroma (Dermal fibrotic papule or small nodule of unknown origin, possibly trauma; appears as a slightly elevated area ~5mm, often with overlying hyperpigmentation and epidermal thickening. When palpated, these are firm and indurated; demonstrate *"dimple sign."*)
question
dark brown elevated, firm, protuberant nodules/plaque usually appearing on earlobes, shoulders, upper chest, and back
answer
Keloids (Exuberant scar tissue due to *excessive proliferation of collagen*, most common in young black people. Appear as *overgrown scars*; pink to dark brown, elevated, firm, protuberant nodules/plaque; *more extensive than the original wound*; irregular claw-like borders. New and active lesions *often itch*. Treat these cautiously due to their high recurrence rate.)
question
pink elevated, firm, protuberant nodules/plaque usually appearing on earlobes, shoulders, upper chest, and back
answer
Keloids (Exuberant scar tissue due to *excessive proliferation of collagen*, most common in young black people. Appear as *overgrown scars*; pink to dark brown, elevated, firm, protuberant nodules/plaque; *more extensive than the original wound*; irregular claw-like borders. New and active lesions *often itch*. Treat these cautiously due to their high recurrence rate.)
question
rubbery, flesh-colored nodule usually seen on trunk, neck, and upper extremities
answer
Lipoma (Benign subcutaneous *fat* tumor, most common in midlife. Appears as freely mobile, rubbery, flesh-colored nodules, only slightly elevated above the skin's surface, but easily palpable deep in skin. Biopsy if rapidly growing; therapy is usually not required, but if desired can be excised.)
question
rubbery, flesh-colored nodule usually seen on trunk, neck, and upper extremities
answer
Lipoma (Benign subcutaneous *fat* tumor, most common in midlife. Appears as freely mobile, rubbery, flesh-colored nodules, only slightly elevated above the skin's surface, but easily palpable deep in skin. Biopsy if rapidly growing; therapy is usually not required, but if desired can be excised.)
question
soft, flesh-colored, protruding papule or nodule DIFFERENTIAL skin tags
answer
Neurofibroma (Focal proliferation of neural tissue in the dermis; multiple lesions are seen in Neurofibromatosis Type 1 [von Recklinghausen's disease]; appear as soft, flesh colored *protruding papule* or nodule which demonstrate characteristic *"buttonhole sign"* [when compressed, the papule feels like it can be pushed through a defect in the skin]; less often, these can be deep, firm nodule [plexiform neurofibroma] and be tender; "feels like bag of worms.")
question
large, deep, firm nodule "feels like a bag of worms"
answer
Plexiform Neurofibroma (Focal proliferation of neural tissue in the dermis; multiple lesions are seen in Neurofibromatosis Type 1 [von Recklinghausen's disease]; most commonly appear as soft, flesh colored *protruding papule* or nodule which demonstrate characteristic *"buttonhole sign"* [when compressed, the papule feels like it can be pushed through a defect in the skin]; less often, these can be deep, firm nodule [plexiform neurofibroma] and be tender; "feels like bag of worms.")
question
yellowish plaques on eyelids
answer
Xanthelasma (Focal collection of *lipid-laden histiocytes* in dermis or tendons with yellow appearance due to fat composition; *usually a skin sign of hyperlipidemia* [not always in case of xanthelasma]. All xanthomas except tendon types are yellow papules, plaques, and nodules.)
question
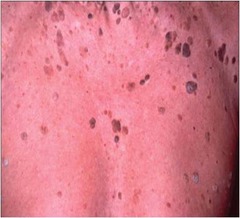
reddish-yellow papules and plaques
answer
Eruptive Xanthomas (*due to very high triglycerides* (Focal collection of *lipid-laden histiocytes* in dermis or tendons with yellow appearance due to fat composition; *usually a skin sign of hyperlipidemia* [not always in case of xanthelasma]. All xanthomas except tendon types are yellow papules, plaques, and nodules.)
question
potato-like nodules commonly seen on elbows, buttocks
answer
Tuberous Xanthoma (Focal collection of *lipid-laden histiocytes* in dermis or tendons with yellow appearance due to fat composition; *usually a skin sign of hyperlipidemia* [not always in case of xanthelasma]. All xanthomas except tendon types are yellow papules, plaques, and nodules.)
question
deep, flesh-colored, hard nodules located within peripheral tendons most commonly involving Achilles tendon and extensor fingers
answer
Tendon Xanthomas (*due to very high cholesterol) (Focal collection of *lipid-laden histiocytes* in dermis or tendons with yellow appearance due to fat composition; *usually a skin sign of hyperlipidemia* [not always in case of xanthelasma]. All xanthomas except tendon types are yellow papules, plaques, and nodules.)
question
, it appears as lower leg lesions. If AIDS-associated, the lesions may appear anywhere.)")
purple macules, papules, plaques, and nodules
answer
Kaposi's Sarcoma (Malignant *vascular tumor caused by HHV8*; appears as *purple* macules, papules, plaques and nodules. In classic Kaposi's Sarcoma (elderly men of Mediterranean descent), it appears as lower leg lesions. If AIDS-associated, the lesions may appear anywhere.)
question
purple macules, papules, plaques, and nodules
answer
Kaposi's Sarcoma (Malignant *vascular tumor caused by HHV8*; appears as *purple* macules, papules, plaques and nodules. In classic Kaposi's Sarcoma (elderly men of Mediterranean descent), it appears as lower leg lesions. If AIDS-associated, the lesions may appear anywhere.)
question
hyperpigmented macules
answer
Freckle/Ephelis (Sun-induced hyperpigmented macules that only occur in sun-exposed areas; very common. *Amount of melanin is increased*, but number of melanocytes stays the same.)
question
 Lentigo simplex: childhood, idiopathic, few in number, (2) Actinic lentigo: adults, *sun induced*, often numerous, more common.)")
hyperpigmented macules
answer
Lentigo (Hyperpigmented macule caused by *increased number of melanocytes* Two main types: (1) Lentigo simplex: childhood, idiopathic, few in number, (2) Actinic lentigo: adults, *sun induced*, often numerous, more common.)
question
hyperpigmented macules
answer
Lentigo (Hyperpigmented macule caused by *increased number of melanocytes* Two main types: (1) Lentigo simplex: childhood, idiopathic, few in number, (2) Actinic lentigo: adults, *sun induced*, often numerous, more common.)
question
light to dark brown macule
answer
Junctional Nevus (Benign common neoplasm of pigment-forming cells [*the nevus cell*], generally having uniform color, surface, and border [changing or symptomatic nevi are suspicious!]. Note that darkening, itching, and development of new nevi are common during pregnancy and adolescence. Types of nevi: (1) Junctional: nevus cells confined to base of epidermis, (2) Compound: nevus cells in epidermis and dermis, (3) Intradermal: nevus cells in dermis only. They vary greatly in appearance and may be any of the following: flat or elevated, smooth or verrucoid, polypoid or sessile, flesh colored to tan to dark brown to blue, often contains hair.)
question
brown, rough-surfaced papule
answer
Compound or Intradermal Nevus (Benign common neoplasm of pigment-forming cells [*the nevus cell*], generally having uniform color, surface, and border [changing or symptomatic nevi are suspicious!]. Note that darkening, itching, and development of new nevi are common during pregnancy and adolescence. Types of nevi: (1) Junctional: nevus cells confined to base of epidermis, (2) Compound: nevus cells in epidermis and dermis, (3) Intradermal: nevus cells in dermis only. They vary greatly in appearance and may be any of the following: flat or elevated, smooth or verrucoid, polypoid or sessile, flesh colored to tan to dark brown to blue, often contains hair.)
question
flesh-colored smooth-surfaced papule
answer
Compound or Intradermal Nevus (Benign common neoplasm of pigment-forming cells [*the nevus cell*], generally having uniform color, surface, and border [changing or symptomatic nevi are suspicious!]. Note that darkening, itching, and development of new nevi are common during pregnancy and adolescence. Types of nevi: (1) Junctional: nevus cells confined to base of epidermis, (2) Compound: nevus cells in epidermis and dermis, (3) Intradermal: nevus cells in dermis only. They vary greatly in appearance and may be any of the following: flat or elevated, smooth or verrucoid, polypoid or sessile, flesh colored to tan to dark brown to blue, often contains hair.)
question
variegated in color; irregular, indistinct border erythematous background
answer
Dysplastic Nevus (Benign common neoplasm of pigment-forming cells [*the nevus cell*], generally having uniform color, surface, and border [changing or symptomatic nevi are suspicious!]. Note that darkening, itching, and development of new nevi are common during pregnancy and adolescence. Types of nevi: (1) Junctional: nevus cells confined to base of epidermis, (2) Compound: nevus cells in epidermis and dermis, (3) Intradermal: nevus cells in dermis only. They vary greatly in appearance and may be any of the following: flat or elevated, smooth or verrucoid, polypoid or sessile, flesh colored to tan to dark brown to blue, often contains hair.)
question
variegated in color; irregular, indistinct border
answer
Dysplastic Nevus (Benign common neoplasm of pigment-forming cells [*the nevus cell*], generally having uniform color, surface, and border [changing or symptomatic nevi are suspicious!]. Note that darkening, itching, and development of new nevi are common during pregnancy and adolescence. Types of nevi: (1) Junctional: nevus cells confined to base of epidermis, (2) Compound: nevus cells in epidermis and dermis, (3) Intradermal: nevus cells in dermis only. They vary greatly in appearance and may be any of the following: flat or elevated, smooth or verrucoid, polypoid or sessile, flesh colored to tan to dark brown to blue, often contains hair.)
question
elevated, dark brown papule or plaque with discrete borders
answer
Congenital Nevus (Benign common neoplasm of pigment-forming cells [*the nevus cell*], generally having uniform color, surface, and border [changing or symptomatic nevi are suspicious!]. Note that darkening, itching, and development of new nevi are common during pregnancy and adolescence. Types of nevi: (1) Junctional: nevus cells confined to base of epidermis, (2) Compound: nevus cells in epidermis and dermis, (3) Intradermal: nevus cells in dermis only. They vary greatly in appearance and may be any of the following: flat or elevated, smooth or verrucoid, polypoid or sessile, flesh colored to tan to dark brown to blue, often contains hair.)
question
elevated, dark brown papule or plaque with discrete borders NOTE large congenital nevi (> 20cm) have increased chance of developing into melanoma
answer
Cognenital Nevus (Benign common neoplasm of pigment-forming cells [*the nevus cell*], generally having uniform color, surface, and border [changing or symptomatic nevi are suspicious!]. Note that darkening, itching, and development of new nevi are common during pregnancy and adolescence. Types of nevi: (1) Junctional: nevus cells confined to base of epidermis, (2) Compound: nevus cells in epidermis and dermis, (3) Intradermal: nevus cells in dermis only. They vary greatly in appearance and may be any of the following: flat or elevated, smooth or verrucoid, polypoid or sessile, flesh colored to tan to dark brown to blue, often contains hair.)
question
irregular in color, surface, border may occur anywhere on body but show predilection for upper back in males and lower legs in females
answer
Superficial Spreading Melanoma (Malignant neoplasm of pigment-forming cells [melanocytes and nevus cells] demonstrating an increasing incidence [1 in 70 lifetime risk]. 50% of melanomas are associated with a nevus. Note that *superficial spreading melanoma is the most common type.*)
question
irregular in color, surface, border may occur anywhere on body but show predilection for upper back in males and lower legs in females
answer
Superficial Spreading Melanoma (Malignant neoplasm of pigment-forming cells [melanocytes and nevus cells] demonstrating an increasing incidence [1 in 70 lifetime risk]. 50% of melanomas are associated with a nevus. Note that *superficial spreading melanoma is the most common type.*)
question
rapidly growing, blue-black, eroded nodule occur anywhere on the body
answer
Nodular Melanoma (Malignant neoplasm of pigment-forming cells [melanocytes and nevus cells] demonstrating an increasing incidence [1 in 70 lifetime risk]. 50% of melanomas are associated with a nevus.)
question
rapidly growing, blue-black, smooth nodule occur anywhere on the body
answer
Nodular Melanoma (Malignant neoplasm of pigment-forming cells [melanocytes and nevus cells] demonstrating an increasing incidence [1 in 70 lifetime risk]. 50% of melanomas are associated with a nevus.)
question
multicolored patch with some elevated areas; changes in size, growing slowly; darkening is insidious (years) occurs on sun-exposed skin
answer
Lentigo Maligna Melanoma (Malignant neoplasm of pigment-forming cells [melanocytes and nevus cells] demonstrating an increasing incidence [1 in 70 lifetime risk]. 50% of melanomas are associated with a nevus.)
question
multicolored patch with some elevated areas; changes in size, growing slowly; darkening is insidious (years) occurs on sun-exposed skin
answer
Lentigo Maligna Melanoma (Malignant neoplasm of pigment-forming cells [melanocytes and nevus cells] demonstrating an increasing incidence [1 in 70 lifetime risk]. 50% of melanomas are associated with a nevus.)
question
irregular, enlarging, black growth occurs on palms, soles, toes or fingers DIFFERENTIAL lentigo maligna melanoma
answer
Acral Lentiginous Melanoma (Malignant neoplasm of pigment-forming cells [melanocytes and nevus cells] demonstrating an increasing incidence [1 in 70 lifetime risk]. 50% of melanomas are associated with a nevus. *Note that acral lentiginous melanoma is most frequent in blacks and Asians.*)
question
irregular, enlarging, black growth occurs on palms, soles, toes or fingers DIFFERENTIAL lentigo maligna melanoma
answer
Acral Lentiginous Melanoma (Malignant neoplasm of pigment-forming cells [melanocytes and nevus cells] demonstrating an increasing incidence [1 in 70 lifetime risk]. 50% of melanomas are associated with a nevus. *Note that acral lentiginous melanoma is most frequent in blacks and Asians.*)
question

Main treatment is surgical excision, with increasing margins for increasing thickness.
answer
Survival Statistics Based on Melanoma Depth
question
shiny, blue-black color, speckled rolled borders; waxy and cratered
answer
Pigmented Basal Cell Carcinoma
question
irregular in color, surface, border
answer
Superficial Spreading Melanoma
question

variegated in color; irregular, indistinct border
answer
Combined Melanocytic Nevus
question
This vesicular eruption is caused by: A. HSV B. VZV C. Poison Ivy D. Streptococcus
answer
C. Poison Ivy Linear and geometric patterns usually have their source outside the body.
question
grouped vesicles on erythematous base
answer
HSV (Grouped vesicles on erythematous base; can quickly become pustules that rupture and crust, which may result in ulcers.)
question
")
grouped vesicles on erythematous base fingers
answer
Herpetic Whitlow (Grouped vesicles on erythematous base; can quickly become pustules that rupture and crust, which may result in ulcers.)
question
generalized skin infection with predisposing skin disease
answer
Eczema Herpeticum (Grouped vesicles on erythematous base; can quickly become pustules that rupture and crust, which may result in ulcers.)
question
Tzanck smear multinucleated giant cells
answer
HSV
question
grouped vesicles in plaque
answer
Chronic HSV
question
 vesicles --> pustules --> crust. Typically all types of lesions seen at the same time 'Dewdrop on a rose petal' is classic.)" alt="Varicella (Caused by primary VZV infection. Crops of macules develop into papules --> vesicles --> pustules --> crust. Typically all types of lesions seen at the same time 'Dewdrop on a rose petal' is classic.)">
vesicles --> pustules --> crust. Typically all types of lesions seen at the same time 'Dewdrop on a rose petal' is classic.)" alt="Varicella (Caused by primary VZV infection. Crops of macules develop into papules --> vesicles --> pustules --> crust. Typically all types of lesions seen at the same time 'Dewdrop on a rose petal' is classic.)">
generalized, pruritic vesicular eruption various lesions (macules, papules, vesicles) "dewdrop on a rose petal"
vesicles --> pustules --> crust. Typically all types of lesions seen at the same time 'Dewdrop on a rose petal' is classic.)" alt="Varicella (Caused by primary VZV infection. Crops of macules develop into papules --> vesicles --> pustules --> crust. Typically all types of lesions seen at the same time 'Dewdrop on a rose petal' is classic.)">
answer
Varicella (Caused by primary VZV infection. Crops of macules develop into papules --> vesicles --> pustules --> crust. Typically all types of lesions seen at the same time 'Dewdrop on a rose petal' is classic.)
question
![Zoster (Caused by reactivation of VZV in sensory nerve; can involve adjacent [*but not bilateral*] dermatomes. Post-herpetic neuralgia is more common in elderly and can be severe.)](https://studyhippo.com/wp-content/uploads/2018/04/zostercaused-by-reactivation-of-vzv-in-sensory-nerve-can-involve-adjacent-but-not-bilateral-dermatomes-post-herpetic-neuralgia-is-more-common-in-elderly-and-can-be-severe.jpg "Zoster (Caused by reactivation of VZV in sensory nerve; can involve adjacent [*but not bilateral*] dermatomes. Post-herpetic neuralgia is more common in elderly and can be severe.)")
unilateral eruption of groups of vesicles along dermatome
answer
Zoster (Caused by reactivation of VZV in sensory nerve; can involve adjacent [*but not bilateral*] dermatomes. Post-herpetic neuralgia is more common in elderly and can be severe.)
question
unilateral eruption of groups of vesicles along dermatome
answer
Zoster (Caused by reactivation of VZV in sensory nerve; can involve adjacent [*but not bilateral*] dermatomes. Post-herpetic neuralgia is more common in elderly and can be severe.)
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
...
question
answer
Superficial desquamation beginning.
question

answer
Superficial desquamation after toxic erythema.
question
answer
...
question
erythematous plaques, violaceous hue; sun exposure DIFFERENTIAL drug reaction
answer
...
question
sparing of the nasolabial folds; "butterfly rash"
answer
...
question
")
redness, warmth, swelling, pain intact epidermis blisters occur only rarely
answer
Cellulitis (displaying the four cardinal signs)
question
answer
Fungal Cellulitis (cannot determine cause by observation)
question
answer
...
question
sharply demarcated red plaque with orange peel appearance (follicles accentuated)
answer
...
question
associated hair follicle
answer
Furuncle
question

no associated hair follicle fluctuates when pressed
answer
Abscess
question
")
red, ill-defined nodules with bruise-like appearance on shins will be painful when touched
answer
Erythema Nodosa (Causes: Strep, OCPs, Pregnancy, or idiopathic)
question
")
sharply demarcated red plaques, later dusky same lesion can reappear prefers the distal extremities, face, lips, and genitalia
answer
Fixed Drug Eruption (Causes: *NSAIDs, sulfonamides,* tetracyclines, carbamazepine)
question
persistent flushing of the face due to high levels of 5HT
answer
Carcinoid Syndrome
question

cutaneous metastases mimicking cellulitis painful, hot
answer
Carcinoma Erysipeloides
question
slightly raised, some blanching at border edematous plaques
<img src="https://chmanchacentro.com/wp-content/uploads/2018/04/urticariaindividual-lesions-last.jpg" title="Urticaria (*Individual lesions last <24 hours*)" alt="Urticaria (*Individual lesions last
answer
Urticaria (*Individual lesions last <24 hours*)
question
localized, acute dermal edema
answer
Uritcaria
question
localized, acute dermal edema geographic patterns
answer
Urticaria, cold induced
question

localized, acute dermal edema
answer
Urticardia, cold induced
question

localized, acute dermal edema
answer
Urticaria, pressure induced
question
answer
...
question
target lesions with rim of pallor and outermost zone of red
answer
(*Most often caused by HSV*)
question
target lesions with rim of pallor and outermost zone of red
answer
(*Most often caused by HSV*)
question
")
slowly expanding, >5 cm red expanding plaque
answer
Erythema migrans (*Caused by Borrelia burgdorferi transmitted by Ixodes*, treat with doxycycline, amoxicillin, or ceftriaxone)
question
slowly expanding, >5 cm red expanding plaque
answer
Erythema migrans (*Caused by Borrelia burgdorferi transmitted by Ixodes*, treat with doxycycline, amoxicillin, or ceftriaxone)
question

answer
Ixodes tick
question
slowly expanding, >5 cm red expanding plaque
answer
Erythema migrans (*Caused by Borrelia burgdorferi transmitted by Ixodes*, treat with doxycycline, amoxicillin, or ceftriaxone)
question
reaction to internal malignancy
answer
Erythema gyratum repens
question

reaction to distal infection? scaling trailing behind red border
answer
Erythema annular centrifugum
question
answer
...
question
answer
...
question
answer
...
question
answer
...

